-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(3): 245-248
doi:10.5923/j.ajmms.20231303.12
Received: Feb. 17, 2023; Accepted: Mar. 13, 2023; Published: Mar. 15, 2023

Description of Pathomorphological Changes of Endometriosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKh. A. Karimjonov1, R. I. Israilov2, A. R. Mamataliev3
1Assistant, Andijan State Medical Institute, Uzbekistan
2Doctor of Medical Sciences, Director of the Republican Pathoanatomical Center of the Ministry of Health of the Republic of Uzbekistan
3Candidate of Medical Sciences, Associate Professor, Head of the Department, Andijan State Medical Institute, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In this study, pathomorphological changes of 80 internal and external endometriosis tissues examined by ARDPA in 2019–22 were studied. In this case, 90–95% internal and 5–10% external endometriosis occur, the process is I st degree 6%, II–level 30%, III–level 50% and IV–level 14%, hyperplastic processes were observed in the endometrium in 54% of cases. Adenomyosis was noted to spread deeply in the pre–climax period, to be accompanied by endometrial hyperplasia of 2–3 degrees, and to develop with benign tumors in ¾ cases.
Keywords: Endometriosis, Adenomyosis, Pathomorphological changes, Hyperplastic processes, Benign tumors
Cite this paper: Kh. A. Karimjonov, R. I. Israilov, A. R. Mamataliev, Description of Pathomorphological Changes of Endometriosis, American Journal of Medicine and Medical Sciences, Vol. 13 No. 3, 2023, pp. 245-248. doi: 10.5923/j.ajmms.20231303.12.
1. Topicality
- In recent years, the number of occurrences of genital endometriosis among gynecological diseases has been increasing [1,2]. In women of reproductive age, endometriosis, according to the data of various authors, is recorded in 12–50% and is manifested along with infertility, chronic pelvic pain syndrome, various somatic diseases [3,4,5,6,7].The aims and objectives of the study are to study pathomorphological changes in adenomyosis and ovarian endometriosis.
2. Materials and Methods
- As the object of the study, 80 internal and external endometriosis tissues, which were examined in the pathology anatomy department of ASMI clinic, ARDPA, MEDICAL–PRO clinic biopsy diagnostic departments over the last 3 years, were taken, in which general morphological–hematoxylin and eosin section was studied by oil painting.
3. Results and Discussions
- When studying the data of internal and external endometriosis tissues in the study, it was found that 90–95% internal and 5–10% external endometriosis were found. In the morphological analysis of these 80 cases, the process in the myometrial layers was I–level 6%, II–level 30%, III–level 50% and IV–level 14%. In histological examinations of the endometrium of patients diagnosed with adenomyosis, hyperplastic processes were observed in 54% of cases. Normal hyperplasia was detected in 86% of patients, and atypical hyperplasia in 14% of patients.In the study, it was found that the syndromes of pain, vegetative and psycho–emotional disorders in adenomyosis develop 2–3,2 times more often than in ovarian endometriosis. In adenomyosis, pain and hemorrhagic syndromes were observed 2,1–2,8 times more often in III–IV stages of the disease, and 1,9–2 times more often in hemorrhagic syndrome–glandular and glandular–stromal variants of the structure of endometrioid foci. The ratio of endometrial hyperplasia, uterine myoma and adenomyosis was 1/1/0,15. Information about endometriosis, endometrioid cysts is rare in young women, and the rate of occurrence increases with age, which helps in the targeted implementation of measures for the treatment and prevention of these diseases.In women, adenomyosis in the pre–climax period has a deep spread, 2–3 degrees, is accompanied by endometrial hyperplasia and develops with good–quality tumors in ¾ cases, and in the post–climax period, the degree of spread is slightly reduced, but with good-quality tumors. it was noted that the growth was parallel, and it was the basis for their clinical diagnosis.According to the result of macroscopic examination of adenomyosis, the shape of the uterus is mostly round, the front and back surface of the organ is enlarged, the consistency is dense, and the surface looks like an uneven marble. It was found that foci were located in the thickened posterior wall in 48 (60%) cases, in the front wall in 13 (16%) cases, and in the fundus of the uterus in 39 (24%) cases. In the section of the myometrium, they were found in the form of small cysts–white tissue branches with a dense consistency, without clear borders, often with hemorrhagic content.
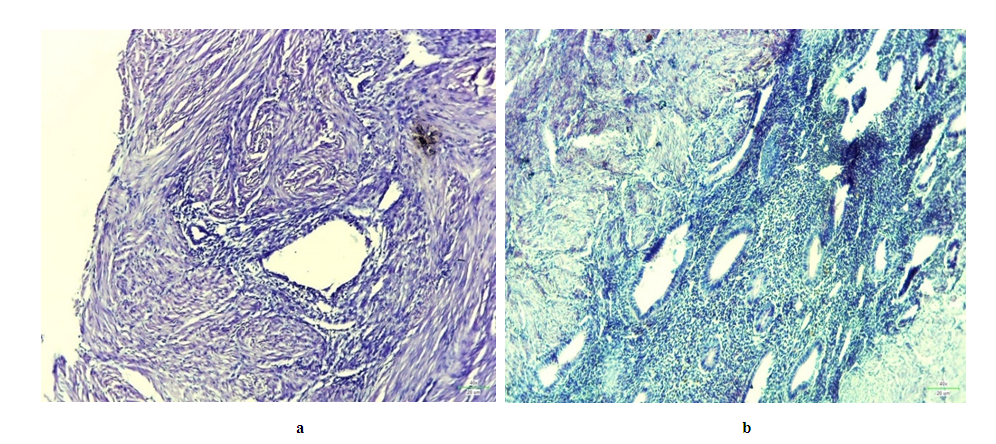 | Figure 1. a, b. Endometrioid foci in diffuse adenomyosis (proliferative phase of menstruation in a woman of reproductive age). Myometrial hyperplasia, glandular–stromal foci of hypertrophied endometriosis. Stained with hematoxylin and eosin, a–x120, b–x200 |
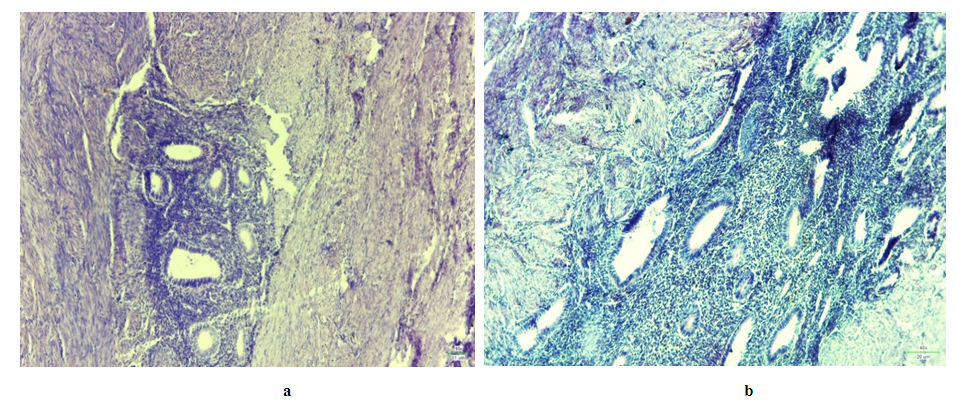 | Figure 2. Adenomyosis of reproductive age – proliferating endometrium. Stained with hematoxylin and eosin, x200 |
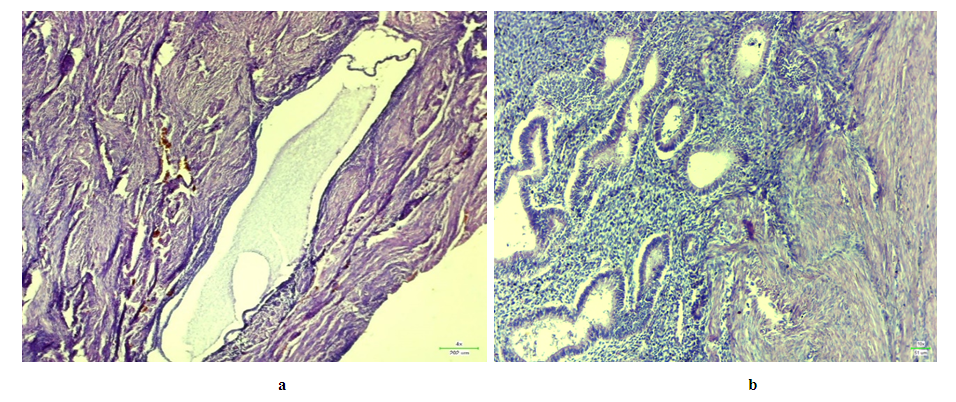 | Figure 3. Foci in adenomyosis. The combination of histological features is mainly glandular, inactive (a) and glandular–stromal, active (b). Stained with hemm. –eosin. a–x120, b–x200 |
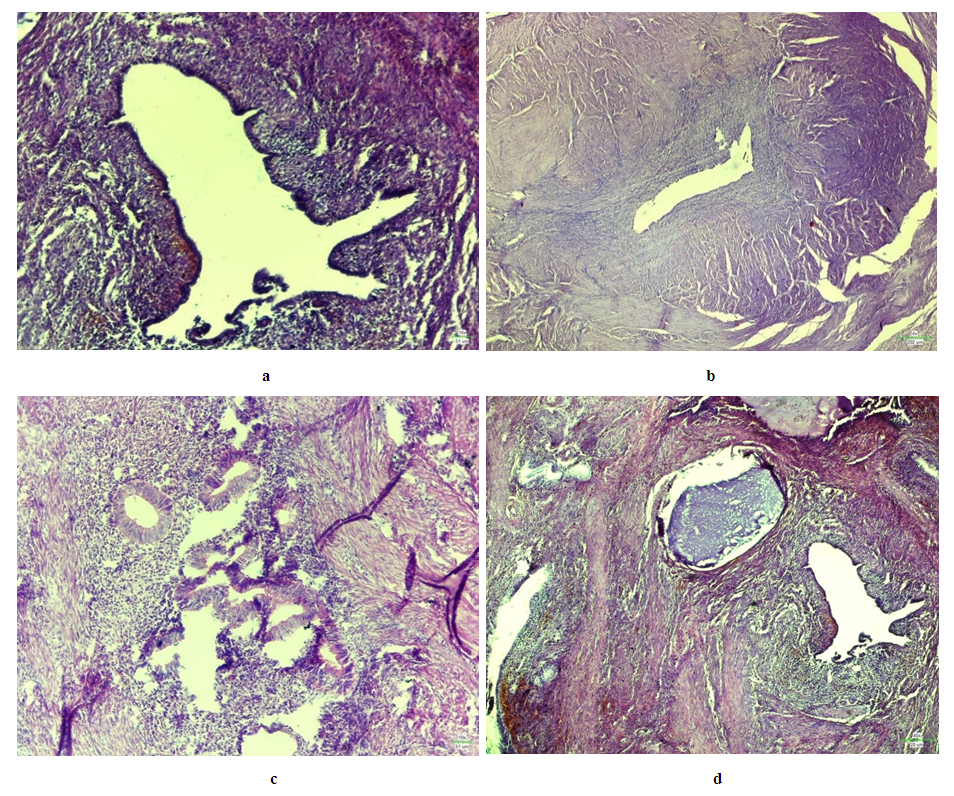 | Figure 4. Ovarian endometriosis in the proliferative phase of the menstrual cycle in women of reproductive age: a, b – wall of endometrioid cysts of irregular shape, covered with epithelium of proliferative and indifferent type (a). cytogenic stroma with foci of hemosiderosis, edema, lymphoid infiltration, (b) epithelium of indifferent type, sclerotic changes, cytogenic stroma with foci of hemosiderosis, c – g proliferative type epithelium among active cytogenic stroma with hemorrhage with a glandular structure, a tumor on the cyst wall, a cuboidal epithelial cyst with a secretory type on the wall of a sclerotic cyst; malignant and sclerosed cytogenic stroma. Staining with hematoxylin and eosin, a, d – x200, b, c – x120 |
4. Conclusions
- Endometriosis is more common in the inner, less outer, myometrial layers, the process is more II–III degree, in many cases it was manifested by simple hyperplasia of the endometrium, less often by atypical hyperplasia. Pain, vegetative and psycho–emotional disorder syndromes, pain and hemorrhagic syndromes in adenomyosis were found to develop more than ovarian endometriosis. The ratio of endometrial hyperplasia, uterine myoma and adenomyosis was 1/1/0.15. Information about endometriosis, endometrioid cysts is rare in young women, and the rate of occurrence increases with age, which helps in the targeted implementation of measures for the treatment and prevention of these diseases.