-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(3): 227-231
doi:10.5923/j.ajmms.20231303.08
Received: Feb. 12, 2023; Accepted: Mar. 6, 2023; Published: Mar. 15, 2023

Evaluation of the Possibility of E-Cadherin, P-Catenin and Cytokeratins Expression in the Diagnostics and Prognosis of the Mammary Gland Accessory Lobe Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLL. T. Alimkhodjaeva, D. A. Nishanov, L. M. Bozarova, M. Kh. Norbekova
Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of our study was to develop new criteria for the differential diagnosis of variants of intraepithelial neoplasia of the mammary gland accessory lobe based on the use of a comprehensive morphological method of investigation using an optimal panel of markers to improve the quality of diagnosis and assessment of invasive cancer risk. Background. Along with breast cancer, the number of cases of the mammary gland accessory lobe cancer has increased in recent years. This trend requires careful screening among women from the high-risk group, which include, first of all, patients with precancerous lesions of the breast. The method of immunohistochemistry in recent years has become widely used by researchers in the study of intraepithelial neoplasia of the breast and its lobe with the aim of early diagnosis and prognosis. Material and methods. The study was based on the results of a retrospective examination of 182 patients with mammary gland accessory lobe cancer. According to the morphological examination results, the patients were divided into 4 groups. The intensity of reactions localized in the cytoplasm and on cell membranes was evaluated by a semi-quantitative method on a point scale from O to 3 using the Leica Q550 image analyzer. Results. In 31 (50.0%) cases of dysplasia the process was located in the right breast, in 27 (43.6%) women - in the left breast, and in 4 (6.4%) cases the lesion was bilateral. There were no significant differences in the location of the pathological process in invasive ductal carcinoma. At invasive lobular carcinoma in situ in 12 (42.9%) cases the pathological process was located on the left, and in 16 (57.1%) cases – on the right. Conclusion. Thus, the expression of cytokeratins 5/6 and 14 types is significantly more often observed in dysplasia (p= 0.0005), which allows them to be used for additional differential diagnosis of dysplasia and highly differentiated carcinomas in situ. Determination of the levels of cytokeratins 5/6, H, cyclin D1, E-cadherin and 3-catenin is the most important tool for the differential diagnosis of various types of breast neoplasia and its additional lobes as an independent factor in assessing tumor invasiveness.
Keywords: Breast cancer, Mammary gland accessory lobe cancer, Immunohistochemistry, Dysplasia, Invasion
Cite this paper: L. T. Alimkhodjaeva, D. A. Nishanov, L. M. Bozarova, M. Kh. Norbekova, Evaluation of the Possibility of E-Cadherin, P-Catenin and Cytokeratins Expression in the Diagnostics and Prognosis of the Mammary Gland Accessory Lobe Diseases, American Journal of Medicine and Medical Sciences, Vol. 13 No. 3, 2023, pp. 227-231. doi: 10.5923/j.ajmms.20231303.08.
1. Introduction
- To date, breast cancer (BC) continues to occupy the first place in the frequency of occurrence among malignant neoplasms in women and is one of the main causes of mortality from cancer. Along with breast cancer, the number of cases of the mammary gland accessory lobe cancer has increased for recent years. The incidence of cancer in the mammary gland accessory lobe makes up 0.2–0.3% of its total frequency [1]. According to most experts, the prognosis of mammary gland accessory lobe cancer (MGALC) is determined by its early diagnosis. This trend requires careful screening among women from the high-risk group, which include, first of all, patients with precancerous lesions of the breast [2-5]. When studying the latest researches on breast diseases, we found that not so much work has been done that gives clear recommendations for diagnosis and treatment, as well as for the prediction of MGALC, which is why this study seems to be relevant and interesting both in terms of clinical and practical oncology [1,6].In recent years, issues of verification and determination of the prognostic value of the so-called pre-invasive breast lesions and its accessory lobe have been intensively developed, among which there are severe dysplasia, in situ breast cancer (carcinoma in situ - CIS), cancer with the onset of invasion [7]. These diseases differ significantly from each other in the course and risk of subsequent development of invasive cancer. E-cadherin, P-catenin and high-molecular-weight cytokeratins are considered the most informative markers that allow a differential diagnosis between ductal and lobular neoplasia of the breast [8-9]. In this regard, the expression of these proteins was studied by us with the aim of confirming the morphological diagnosis and determining their diagnostic specificity. First of all, E-cadherin, a transmembrane protein, which is an adhesion protein, belongs to the markers of differential diagnosis. Loss of membrane expression of E-cadherin is considered a hallmark of lobular neoplasia, while most ductal carcinomas and dysplastic lesions, as well as normal ductal epithelium, are highly protein-expressing. However, the occasional loss of E-cadherin expression in ductal carcinoma cells, as well as aberrant protein expression in lobular neoplasia, can lead to diagnostic errors [10]. In such cases, a number of researchers use additional markers, such as high-molecular cytokeratin, specific for lobular neoplasia cells, and alpha, beta and gamma-catenins which are specific for ductal cells. The method of immunohistochemistry has become widely used by researchers in the study of intraepithelial neoplasia of the breast and its lobe for early diagnosis and prognosis in recent years [2,11]. The immunohistochemical method (IHC) allows not only to determine the histogenetic features of precancerous lesions of the mammary gland and its additional lobe, the expression of hormonal receptors, various oncoproteins, proliferative activity, but also to identify the presence of minimal invasion, often significantly changing the prognosis of the disease. In this regard, the IHC method has become widely used by researchers in the study of intraepithelial neoplasia of the mammary gland and its lobe. However, in most published studies using this method, a limited number of markers does not allow to fully clarify the biological profile of the studied diseases. There is no data on the prognostic significance of these types of neoplasia. A comprehensive diagnostic algorithm combining morphological and immunohistochemical criteria has not been determined [12]. All of the above mentioned testifies to the high relevance of developing criteria issue for the verification of pre-invasive breast and its accessory lobe diseases for oncology and pathological anatomy and determines the need for additional research in this direction.The aim of our study was to develop new criteria for the differential diagnosis of intraepithelial neoplasia variants of the mammary gland accessory lobe based on the use of a comprehensive morphological method of investigation using an optimal panel of markers to improve the quality of diagnosis and assessment of invasive cancer risk.
2. Material and Methods
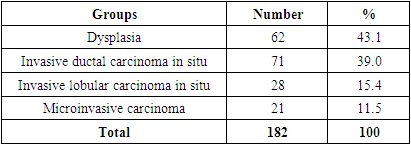
- Our study was based on the results of a retrospective examination of 182 patients with mammary gland accessory lobe cancer treated at the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology from 2010 to 2020. According to the morphological examination results, the patients were divided into 4 groups. The 1st group included 62 (34.1%) patients with severe dysplasia, which was defined below as "dysplasia". The 2nd group consisted of 71 (39.0%) patients with ductal carcinoma in situ, hereinafter referred to as " invasive ductal carcinoma (IDC)". The 3rd group included 28 (15.4%) women with lobular carcinoma in situ, hereinafter referred to as "invasive lobular carcinoma (ILC)". The 4th group included 21 patients (11.5%) with carcinoma in situ with the onset of invasion, this group was designated as "microinvasive carcinoma ". It is usually referred to as DCIS with microinvasion (Tab.1).
|
3. Results
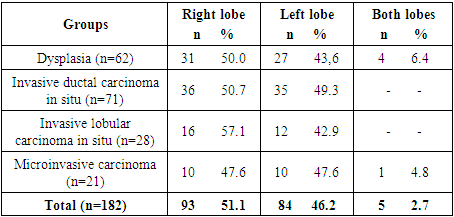
- In 31 (50.0%) cases of dysplasia the process was located in the right breast, in 27 (43.6%) women - in the left breast, and in 4 (6.4%) cases the lesion was bilateral. There were no significant differences in the location of the pathological process in invasive ductal carcinoma: in 35 (49.3%) patients the lesion was found in the left mammary gland and in 36 (50.7%) cases - in the right one. A similar pattern was observed at microinvasive carcinoma in situ: in 10 (47.6%) cases the lesion was located on the left, in 10 (47.6%) - on the right, and in 1 (4.8%) case the lesion was bilateral. At invasive lobular carcinoma in situ in 12 (42.9%) cases the pathological process was located on the left, and in 16 (57.1%) cases – on the right (Tab.2).
|
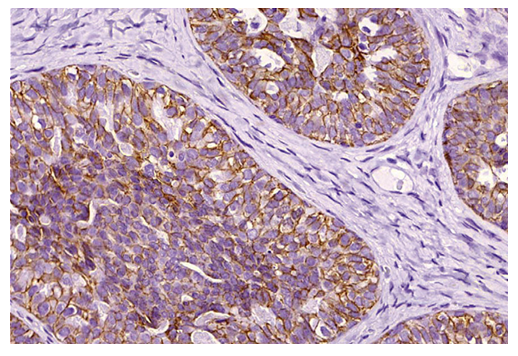 | Figure 1. Positive expression of E-cadherin in ductal carcinoma in situ. х400 |
 | Figure 2. Expression of E-cadherin in the studied samples. х400 |
 | Figure 3. Expression of P-catenin in the studied samples. х400 |
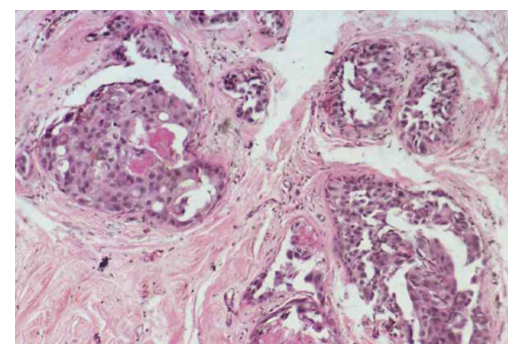
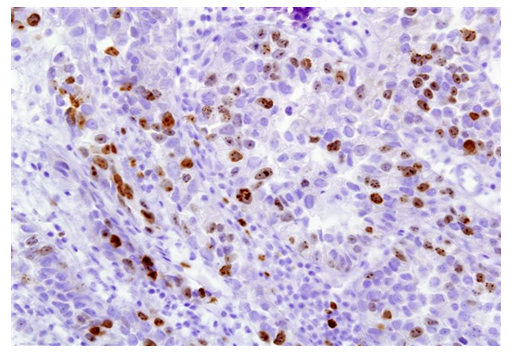
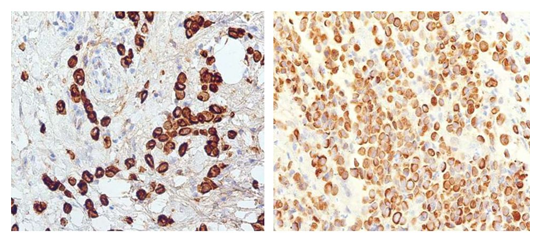 | Figure 4. Positive cytoplasmic expression in tumor cells of the mammary gland accessory lobe of total cytokeratins (left) and high-molecular cytokeratins (right). х200 |
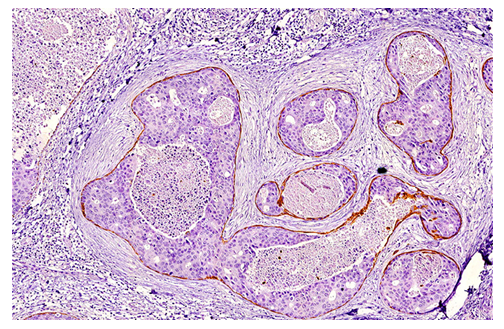 | Figure 5. Expression of cytokeratin types 5/6 by myoepithelial cells in case of intraductal carcinoma in situ. х200 |
4. Conclusions
- Thus, the expression of cytokeratins 5/6 and 14 types is significantly more often observed in dysplasia (p= 0.0005), which allows them to be used for additional differential diagnosis of dysplasia and highly differentiated carcinomas in situ. E-cadherin proved to be highly specific as a marker characteristic of intraductal carcinoma; its expression was determined significantly more often in this type of tumor (р= 0.0005). Obviously, these markers cannot be used for differential diagnosis between lobular and ductal carcinomas in situ, since there are no significant differences in their expression in these types of neoplasia. However, they allow us to further characterize the lesion: in all positive cases, there was also no expression of receptors for estrogen and progesterone, which allowed them to be attributed to the basal cell type of cancer in situ.Histological examination of precancerous lesions of the mammary gland should be supplemented with an assessment of the expression of immunohistochemical markers. Determination of the levels of cytokeratins 5/6, H, cyclin D1, E-cadherin and P-catenin is the most important tool for the differential diagnosis of various types of breast neoplasia and its accessory lobes as an independent factor in assessing tumor invasiveness.The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.