-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(3): 203-206
doi:10.5923/j.ajmms.20231303.02
Received: Feb. 19, 2023; Accepted: Feb. 28, 2023; Published: Mar. 10, 2023

The Course of Juvenile Idiopathic Arthritis and Kidney Damage
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimdjanov Ilhamdjan Asamovich1, Madaminova Malika Shavkatovna2, Dinmukhammadieva Dilorom Rakhimzhanovna2
1Heads the Department of Children's Diseases in Family Medicine, Tashkent Medical Academy, Tashkent, Uzbekistan
2Basic Doctorant of the Department of Children's Diseases in Family Medicine, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Karimdjanov Ilhamdjan Asamovich, Heads the Department of Children's Diseases in Family Medicine, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study of the course of juvenile idiopathic artritis (JIA), determination of disease activity, duration, number of affected joints and target organs improved the understanding of the pathogenesis of the disease and made it possible to better characterize the reliability of use in therapy. The aim of the study was to research various variants of the course of JIA and kidney damage.Tested 38 patients aged 3 to 17 years with JIA and a questionnaire, clinical, anamnestic and laboratory-instrumental examination were conducted. Results of the study showed that 29-76.3% patients characterized criteria as arthritis lasting 3 months or more, morning stiffness, arthritis of the second joint that arose after 3 months and later, symmetrical damage to small joints, effusion into the joint cavity. In 28.9% patients, a persistent variant of oligoarthritis was noted, and progressive oligoarthritis occurred in 71% of the examined patients. In 60.5% patients, the disease proceeded with kidney damage. The duration of the course in JIA in children ranges from 3 months to 8 years, large and medium joints are more often affected - knee, ankle, wrist, elbow, hip. The exudative component of 39% is less pronounced in boys, productive-dystrophic changes of 61% in the joints of the lower extremities predominate. In girls, exudation in the joints of the upper extremities prevailed - 85%. Kidney damage in the form of nephritis was observed in 60.5%, microalbuminuria - in 13.2%, an increase of creatinine data in the blood – 68%.
Keywords: Juvenile idiopathic arthritis, Children, Damage, Kidney, Glomerulonephritis, Acute or chronic interstitial nephritis
Cite this paper: Karimdjanov Ilhamdjan Asamovich, Madaminova Malika Shavkatovna, Dinmukhammadieva Dilorom Rakhimzhanovna, The Course of Juvenile Idiopathic Arthritis and Kidney Damage, American Journal of Medicine and Medical Sciences, Vol. 13 No. 3, 2023, pp. 203-206. doi: 10.5923/j.ajmms.20231303.02.
Article Outline
1. Introduction
- Juvenile idiopathic arthritis (JIA) is a destructive and inflammatory joint disease with unknown etiology, complex immunoaggressive pathogenesis, which is characterized by symmetrical chronic arthritis, systemic damage to internal organs, leading to disability in sick children [1]. In this regard, the problem of improving the efficiency of correction optimization in JIA remains extremely relevant, both from the point of view of scientific and practical pediatrics. The leading risk factors for reduced life expectancy in JIA are diseases of the cardiovascular system, damage to the urinary tract, gastrointestinal tract, infections, and lymphoma [3]. Kidney pathology occurs in JIA with a high frequency - from 57 to 73% according to different authors [8]. With this disease, urinary tract infections, cystitis, pyelonephritis, glomerulonephritis, secondary amyloidosis of the kidneys, acute or chronic interstitial nephritis, chronic kidney disease, papillary necrosis, vasculitis of the renal vessels can be observed. In most patients with JIA, kidney damage determines the prognosis and outcome of the disease [4]. Idiopathic arthritis is a systemic disease that can affect internal organs. In most cases, this is due to the kidneys. Kidney damage in idiopathic arthritis is the most common cause of death from this disease [6]. There are kidney lesions that are directly related to the disease itself, and iatrogenic lesions that are associated with the effects of drug therapy. And often, treatment for juvenile idiopathic arthritis hastens or precipitates kidney damage. Glucocorticoids and cytostatics reduce renal function, which leads to their diseases [5]. Most drugs used to treat JIA can cause kidney damage. This is due to their direct nephrotoxic effect or through the body's immune response mechanisms [7]. To assess the severity of renal damage in autoimmune diseases, it is recommended to use the index of chronicity as an additional indicator. If the chronicity index is high, kidney changes are irreversible, immunosuppressive therapy is ineffective, and this, in turn, is considered a poor prognostic sign. Changes in the kidneys are usually diffuse in nature with an outcome in chronic renal failure and renal amyloidosis [11]. All this dictates the need to optimize early diagnosis, prognosis, correction and prevention of complications from the urinary system in juvenile idiopathic arthritis. Kidney damage in JIA occupies a special place among other systemic manifestations of this disease and has a huge impact on the prognosis of the disease, approaches to its therapy, and outcome [9]. According to various authors, renal pathology occurs in 20-75% of patients with this disease [10]. In terms of the frequency of kidney damage, JIA ranks third among rheumatic diseases, second only to such diseases as SLE and SV.The structure of rheumatoid nephropathy is diverse and includes changes that are either pathogenetically associated with the disease itself (secondary amyloidosis, glomerulonephritis, tubulointerstitial nephritis (TIN)), or as an extra-articular manifestation (renal vasculitis), or associated with drug therapy. Renal changes are characterized by the early onset of non-sustained leukocyturia and mild proteinuria and hematuria, and are most often observed at the onset of the disease or during its exacerbation, and are also associated with the activity and severity of JIA [2].The aim of this study was to study various variants of the course of JIA and kidney damage.
2. Materials and Methods of Research
- To determine the nature of kidney damage in patients with juvenile idiopathic arthritis, 38 children with JIA were examined and a questionnaire, clinical, anamnestic and laboratory-instrumental examination were conducted. The studies were carried out on the basis of the cardio-rheumatology department of the Tashkent medical academy multidisciplinary clinic. Of the 38 patients, there were 20 (52.7%) girls and 18 (47.3%) boys aged 3 to 17 years (mean age 10 years). The duration of the disease ranged from 3 months to 8 years. Girls predominated among the examined patients depending on gender. The great number of patients (more than 50%) were children with a disease period of up to 1 year, more than 5 years of disease was in 2 observed children. The timing of diagnosis ranged from 4 months to 3 years. The diagnosis was established in accordance with the classification of juvenile idiopathic arthritis according to the second version of ILAR "International League of Associations for Rheumatology" and ICD-10. Despite the sufficient clarity of the criteria for early diagnosis of JIA, more than a year to diagnose the disease in the patients we observed in more than a third of cases, and only 13 (34.2%) patients were diagnosed intime. Considering the aggressiveness of the course of JIA, the timing of the diagnosis is important, because timely treatment leads to a further favorable prognosis of the disease.
3. Research Results and Discussion
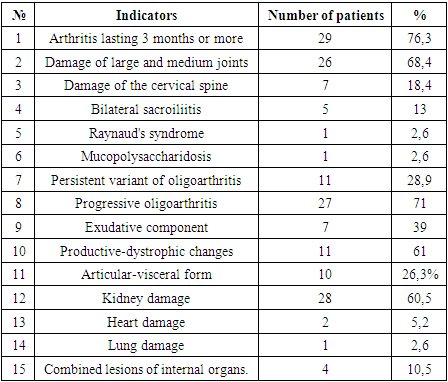
- We analyzed the frequency of occurrence of diagnostic clinical criteria for JIA among the examined groups of patients. The absolute majority of the examined patients (29-76.3%) were characterized by such criteria as arthritis lasting 3 months or more, morning stiffness, arthritis of the second joint that arose after 3 months and later, symmetrical damage to small joints, effusion into the joint cavity. In the affected joint, pain, swelling, deformity and limitation of movement, an increase in local skin temperature were noted. Large and medium joints were more often affected - in 26 (68.4%) knee, ankle, wrist, elbow, hip joints. In 7 (18.4%) patients there was a lesion of the cervical spine, in 5 (13%) patients bilateral sacroiliitis, in 1 (2.6%) the disease was accompanied by Raynaud's syndrome and in 1 (2.6%) the patient was accompanied by a genetic disease mucopolysaccharidosis, Hunter type (table 1).
|
|
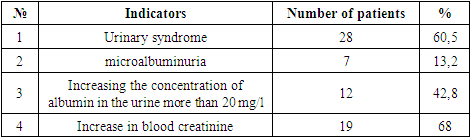
4. Conclusions
- 1. The duration of the course in JIA in children ranges from 3 months to 8 years, large and medium joints are more often affected - knee, ankle, wrist, elbow, hip. Persistent course was noted in 28.9% of the patients, and a progressive course- in 71%.2. The course of the features of the articular syndrome by sex showed that the exudative component of 39% is less pronounced in boys, productive-dystrophic changes of 61% in the joints of the lower extremities predominate. In girls, exudation in the joints of the upper extremities prevailed - 85%. The average age of the patients was 7 years, X-ray was determined mainly II degree according to Steinbrokker.3. Kidney damage in the form of nephritis was observed in 60.5%, microalbuminuria - in 13.2%, an increase in the concentration of creatinine in the blood – 68%.