Shukhrat Kh. Ziyadullayev1, Sayyora Kh. Yuldasheva2
1Samarkand State Medical University, Uzbekistan
2Tashkent Medical Academy of Urgench Branch, Uzbekistan
Correspondence to: Sayyora Kh. Yuldasheva, Tashkent Medical Academy of Urgench Branch, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Asthma is one of the most common chronic inflammatory disorders, associated with reversible airflow obstruction, airway hyperresponsiveness, and airway remodeling. This disease has a significant impact on individuals, their families, and society. Standardized therapeutics such as inhaled corticosteroid in combination with long acting β2 agonist have been applied for asthma control; however, complementary and alternative medicines, especially herbal medicines, are still widely used all over the world. A growing body of literature suggests that various herbals or related products might be effective in inhibiting asthmatic inflammation. In this review, we summarize recent advances about the mechanistic studies of herbal medicines on allergic airway inflammation in animal models and their potential application into clinic for asthma control.
Keywords:
Bronchial asthma, Mucoactive phytopreparations, Cough, Acute respiratory diseases
Cite this paper: Shukhrat Kh. Ziyadullayev, Sayyora Kh. Yuldasheva, The Effectiveness of Phytotherapy in Complex Therapy of Bronchial Asthma, American Journal of Medicine and Medical Sciences, Vol. 13 No. 2, 2023, pp. 107-111. doi: 10.5923/j.ajmms.20231302.17.
1. Relevance
It is known that acute respiratory diseases (ARI) occupy the first place among acute respiratory tract infections (OP) in both children and adults. ARI is a group of multicharacter deseases, resulting from exposure to the respiratory tract of various viral and bacterial agents, tropical for the epithelium of the respiratory tract. Respiratory syncytial viruses predominate among viruses, viruses of flu, parafluenza and adenoviruses. Respiratory viruses can support chronic diseases of the respiratory system, especially bronchial asthma and chronic obstructive pulmonary disease. It has been shown that the viral defeat of the malignant bronchi leads to an increase in the perception of allergens and pollutants, an increase in the production of bioactive substances and exacerbation of desease. Most causative agents of bacterial acute respiratory infections are part of the opportunistic bacterial microbiota is ubiquitous in the human respiratory tract. Therefore, in the mechanisms of pathogenesis of these diseases, the initiating and decisive factor is an acute decrease in local and general protection factors as a result of exposure to the virus. Such a clinical situation is observed in the formation of viral bacterial associations [1].At the same time, the respiratory system is a complex multifunctional system. The mucous membranes of the respiratory tract are constantly exposed to various potentially pathogenic substances that a person inhales with air. There are many protective mechanisms that determine the warming, moisturizing and cleansing of the respiratory tract from foreign substances. Currently, there are three main mechanisms for removing inhaled and airborne products.• Mucociliary clearance (MCC).• Cough – insufficient action.• Alveolar clearance – removal of insoluble particles deposited on the respiratory surface of the lungs.Mucociliary clearance is the process of clearing mucus due to the movement of cilia. The MCC consists of two components: the ciliary apparatus of the ciliated epithelium and the secretory system of DP, including secretory cells, submucosal protein-mucous glands and mucus layer, secreted by those that cover the epithelium of DP. The liquid lining the DP consists of two layers: a layer of silica or periciliary fluid, a layer of porous resins, and a layer of superior mucin (see pic.). The surrounding liquid, the sol layer, is a low—viscosity solution that allows the cilia to vibrate at high frequencies and protects the surface of epithelial cells from mucins covering them. The mucin layer (gel layer) is represented by mucoproteins (high-molecular glycoproteins produced by goblet cells). The structure of secreted mucins and the chemical properties of their surface groups determine the viscosity and elasticity of bronchial secretions. The chemical composition of the gel layer determines the antibacterial and antiviral activity of secretory immunoglobulins (sIgA), lysozyme, lactoferrin and other bioactive substances included in its composition.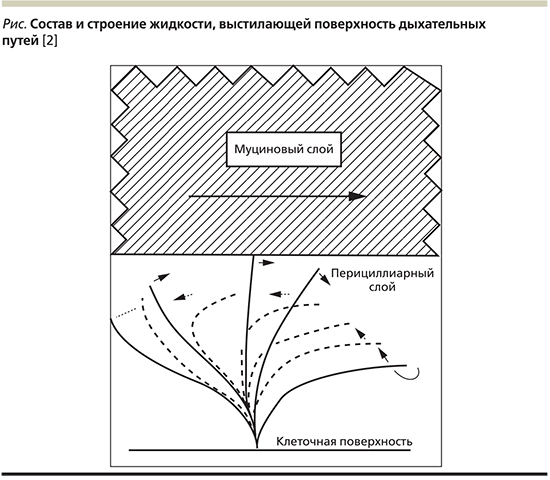 | Pictue 1. Composition and structureof the fluid lining the surface of the respiratory tract |
MCC dysfunction is caused by defects in the ciliary body or secretory components, which leads to a decrease in the physical, chemical and biological protection of the respiratory tract. If the MCC is ineffective, a cough occurs and the airways are cleaned [2].Currently, herbal preparations for the treatment of acute inflammatory diseases of the respiratory tract are actively used both in Russia and abroad. So, in 2014, the results of his research were published by Yoo Du interviewed 17,650 children (and their parents) and adolescents in Germany.Acute respiratory infections [3].Eucabal syrup summarizes the positive effects on the respiratory tract inherent in psyllium and thyme extracts, which determine its high effectiveness. The greatest experience in the use of phytopreparations, especially its Eucabal syrup, in acute respiratory diseases has been accumulated in pediatric practice [4]. The results of research conducted on the basis of the City Clinic Hospital of Botkin and Mukhin in 2016, the results confirmed the high efficacy of Eucabal syrup in the treatment of patients with acute viral sinusitis complicated by tracheobronchitis is used as a drug therapy. On the fifth day of treatment, the effectiveness of monotherapy was assessed as remission in 75% of patients, combined therapy, including decongestants and nasal sprays based on seawater, 82.6% of patients recovered, and 17.4% recovered. The treatment was well mastered, there were no side effects [5]. Eucabal balm is used as an ingredient for scrubbing, steam inhalations or therapeutic baths and potential use in patients with allergic rhinitis [6].Viral infections can contribute to the development of complications such as bronchitis, laryngitis, tracheitis, medium otitis, pneumonia, encephalitis, bronchial asthma. It should also be borne in mind that the younger the child, the greater the likelihood of complications. The peak incidence of acute respiratory diseases (ARI) in children falls at 6 months of age. Up to 6 years, from 4 to 10 diseases per year. This is facilitated by anatomical immaturity, features of the physiology of the bronchopulmonary tree, features of the immune system in childhood. Thus, the bronchopulmonary system of a child has unique age-related features of short nasal passages, immaturity of surfactant and insolvency of alveoli (the final formation of acinuses occurs by 5-9 years). All of these factors in the composition of the previous characteristics of the immune system in children (decrease in the formation of endogenous interferon, secretory immunoglobulin A, nasal secretory lysozyme) can lead to the formation of the eyes of chronic infection. Chronic diseases of the nasopharynx and lungs, bronchial asthma (BA), a more frequent and severe group with allergic rhinitis, the frequency of glomerulonephritis and many other groups of diseases are common among sick children, was noted that they are much more often detected in higher [7].As noted above, herbal preparations should be considered as a treatment option for a less severe cough that occurs with acute laryngitis, tracheitis and/or bronchitis. The main properties that they should have: expectorant, anti-inflammatory, mucoregulatory. Many herbal preparations meet these requirements: eucalyptus, licorice root, plantain, coltsfoot (lat.Tussilago), thyme, primrose, ivy leaves, marshmallow root, rosemary, chamomile and others. In addition to use in acute respiratory diseases, herbal preparations are positioned for the treatment of chronic infections, prevention of exacerbations and complex treatment [8-10].The most sensitive reflex zone in the respiratory tract is the laryngeal surface of the epiglottis; anterior interstitial surface of the larynx; the area of the vocal cords and the sublingual space; bifurcations of the trachea and lobar bronchi. At the same time, the density of cough receptors decreases towards the distal part of the bronchial tree. At the same time, they become more sensitive to cough-provoking stimuli. The impulse, emerging in the irritant reflective zone, is transmitted by an affective volok to the cough center, which is in the extended brain, is closed by efferent fibers of the recurrent laryngeal, diaphragmatic and spinal nerves leading to effector muscles (thoracic, diaphragmatic and abdominal) [11]. Over the past decades, research on medicinal plants and their folk use has expanded in various parts of Pakistan. In recent years, a large amount of information has been documented about the use of plants in local treatment systems by both ethnic peoples and rural communities around the world, and the number of Pakistanis is growing. A holistic approach based on experience contributes to the discovery of safe, new and affordable medicines. The United States has a long history of developing natural medicines, and in 1991, almost half of the best-selling medicines were natural products or their derivatives. With the passage of time, the importance of botanical research increases every day, and more and more convincing evidence is being collected confirming the widespread use of medicinal plants in TM. Over the past five years, about 13,000 plants have been studied [12]. Many species of the Compositaceae family are usually identified as weeds found in a built-up environment, and are among the first species to appear in the field after preparing the soil for planting. This may contribute to the high citation of species of this family in rural areas, where the main source of medicinal plants are household plots [13]. Interest in acute respiratory viral infections (ARVI), including influenza and the new coronavirus disease (COVID-19), is associated with the high prevalence of these diseases and their medical and social significance. Thus, according to the World Health Organization (WHO), ARVI accounts for 90-95% of all infectious diseases [14]. In Russia, more than 30 million people are infected annually, and the annual economic damage is estimated at 60 billion rubles. (approximately 80% of all losses from infectious diseases) [15,16]. Although the medical and economic consequences of the COVID-19 pandemic have yet to be assessed, it is clear that these losses will be huge [17]: exacerbation of sinusitis, tracheitis, acute bronchitis, pneumonia, chronic obstructive pulmonary disease (COPD). Bacterial infections often occur against the background of viral suppression of the immune system. Elderly patients and persons with chronic diseases are at high risk of developing complex acute respiratory infections [18,19]. The analysis of literary sources allowed us to establish the diverse and complex influence of medicinal plants on the course of the disease. It has a direct effect on the process of stone formation, stabilization of the ionic strength of urine and inhibitors of stone formation, acceleration of the passage of stone, its fragments and sand after successful destruction by remote lithotripsy. Known side effects [20]. And the effectiveness is confirmed by both time and scientifically based methods. Replenishment of the range of pharmaceutical preparations containing high-quality biological compounds of plant origin is an urgent task, as the demand for them is growing rapidly. Phytopreparations containing biologically active substances are combined for treatment on the pharmaceutical market of the Russian Federation. It has antispasmodic, antiseptic, anti-inflammatory and diuretic properties, promotes the removal and dissolution of stones. [21-23]The purpose of the study was to evaluate the possibility of using licorice root in the complex therapy of bronchial asthma.Objectives of the research: to determine the effectiveness of the medicinal plant "licorice root" in the complex therapy of bronchial asthma.
2. Methods of the Research
Fourty patients with bronchial asthma were examined at the Department of Pulmonology at the OMMPC for two months. Gender and age were divided randomly. The first twenty patients (group 1) were treated exclusively with medication.The rest twenty patients (group 2) combined treatment, medication + phytotherapy.
3. Medical Treatment
For patients with BA, except for high doses of combined IGCS/DDBA drugs there is an additional therapy, which includes tiotropium bromide, biological drugs and systemic GCS.Tiotropium bromide (TB) in the Respimat delivery system (Spiriva Respimat) was prescribed to patients with severe BA and uncontrolled symptoms while taking IGCS or IGCS / DDBA; with persistent frequent or severe asthma exacerbations; patients with fixed bronchial obstruction (i.e., the ratio of FEV1 / FVC – forced vital capacity of the lungs <0.7 after a bronchodilator test), concomitant chronic obstructive pulmonary disease (COPD), if there are restrictions on the use of DDBA. Additional indications for the appointment of TB can be smoking, the predominance of nocturnal symptoms of AD and a positive bronchodilation test with CDBA in patients with uncontrolled AD [13].Combined treatment (medication + herbal medicine)The remaining 20 patients, in addition to the above mentioned drug treatment, received additional phytotherapy:1. Licorice naked (roots) should be taken in the form of an infusion of 1/4–1/3 cup 3-5 times a day after meal with bronchospasm.
4. Results
In patients who received combined treatment, symptoms were cured 40% faster. There was an improvement in the state of health. Not significant side effects in the form of headaches, dizziness, vomiting, occurred in the second group of patients by 23% less than in the first group of patients who received exclusively medical treatment. Conclusion: It turned out that the combined treatment of AD is effective, provided that caution is observed in calculating doses.
References
| [1] | Isakov V.A., Isakov D.V., Belyaeva T.V., Vodeyko L.P. Prospects of therapy of respiratory infections. Practical pulmonology. 2015; 1: 14–21. |
| [2] | Amelina E.L., Anaev E.H., Krasovsky C.A. and others. Mucoactive therapy. M., 2006. pp. 7-41. |
| [3] | Dui., Wolf I.-K., Zhuang V. and others. The use of herbal medicines among children and adolescents in Germany. Set. Alternatively. Medicine. 2014; 14(218): 13. |
| [4] | Blazhko V.I., Dementieva Ya.V. Cough: modern approaches to diagnosis and treatment. Acute and urgent conditions in the practice of a pediatrician. 2012; 6(33): 63–8. |
| [5] | Miserickiy Yu. L., Melnikova I. M. place herbal preparations in therapy cough in children. RMJ. 2017; 5: 324-6. |
| [6] | Ovchinnikov A.Yu., Miroshnichenko N.A., Ekaterinchev V.A., Smirnov I.V. Upper respiratory tract infections in children and adults. RMZH. 2016; 26: 1739-42. |
| [7] | Medical virology / Edited by D.K. Lvova. M.: MIA, 2008. pp. 381-386. |
| [8] | Ram A., Balachandar S., Vijayanant P., Singh V.P. Medicinal plants useful for the treatment of chronic obstructive pulmonary disease (COPD): current state and prospects for the future // Phytotherapy.2011. Volume 82(2). pp.141–151. |
| [9] | Go R., Pittler M.H., Ernst E. Herbal medicines for COPD treatment: a systematic review // Eur. Respir. J. 2006. Volume 28(2). pp. 330-338. |
| [10] | Gao Z., Liu Yu., Zhang J., Upur H. The effect of Jianpi therapy in the treatment of chronic obstructive pulmonary disease: a systematic review // J. Tradit. Rank. Med. 2013. Volume 33(1). pp. 1-8. |
| [11] | Alasmari A. Phytomedicinal potential characterization of medical plants (Rumex nervosus and Dodonaea viscose). J. Biochem. Tech. 2020; 11(1): 113-21. |
| [12] | Karou D, Nadembega WMC, Ouattara L, Ilboudo DP, Canini A, Nikiéma JB, Simpore J, Colizzi V, Traore AS. African ethnopharmacology and new drug discovery. Med Aromat Plant Sci Biotechnol. 2007; 1(1): 61–69. |
| [13] | Daehler CC. Taxonomic distribution of invasive angiosperms: ecological data and comparison with agricultural weeds. Biol Conserv. 1998; 84(2): 167–180. |
| [14] | Influenza. WHO, 2018. Access: https://www.who.int/ru/news-room/factsheets/detail/influenza -(seasonal) (accessed 01.10.2021). [Flu. World Health Organization, 2018. Available at: https://www.who.int/ru/news-room/factsheets/detail/influenza -(seasonal) (access date – 01.10.2021) (In Russian)]. |
| [15] | On the state of sanitary and epidemiological welfare of the population in the Russian Federation in 2016: state report. Federal Service for Supervision of Consumer Rights Protection and Human Well-being. M. 2017; 220 p. [About the state of sanitary and epidemiological welfare of the population in the Russian Federation in 2016: state report. Federal Service for Supervision of Consumer Rights Protection and Human Well-Being. Moscow. 2017; 220 p. |
| [16] | Yushchuk N.D., Khadartsev O.C. Prevention of influenza and acute respiratory viral infections, taking into account the peculiarities of their epidemic process. Infectious diseases: news, opinions, training. 2018; 2: 44–51. [Yushchuk N.D., Khadartsev O.C. Prevention of influenza and acute respiratory infections and features of their epidemic process. Infectious diseases: news, opinions, education=Infectious diseases: news, views, education. 2018; 2: 44–51. |
| [17] | Kolbin A.C., Gomon Yu.M., Balykina Yu. and others. Socio-economic and global burden of COVID-19. Qualitative clinical Practice. 2021; 1:24-34. [Kolbin A.C., Gomon Y.M., Balykina Y.E. and others. Socio-economic and global burden of COVID-19. High-quality clinical practice = Proper clinical Practice. 2021; 1:24-34]. |
| [18] | Watkins K., Sridhar D. Pneumonia: a global cause without champions. The Lancet. 2018; 392(10149): 718–19. doi: 10.1016/S0140-6736(18)31666-0. |
| [19] | Vertkin A.L., Prokhorovich E.A., Namazova L.C. and others. Optimization of empirical therapy of community-acquired pneumonia in elderly and senile patients. RMJ. 2002; 16: 708-712. [Vertkin A. L., Prokhorovich E. A., Namazova L. C. and others. Optimization of empirical therapy of community-acquired pneumonia in elderly and senile patients. Russian Medical Journal = Russian Medical Journal. 2002; 16: 708-712 (in Russian)]. |
| [20] | Hite GJ, Mishvelov AE, Melchenko EA, Vlasov AA, Anfinogenova OI, Nuzhnaya CV, Kukharuk MY, Bledzhyants. GA, Osadchiy SS. Holodoctor Planning Software Real-Time Surgical Intervention. PHARMACOPHORE, 2019; 10(2): 1-12. |
| [21] | Borisov VV, Koptev VV, Enaleeva SK, Demerza YuA. Shed in the treatment and prevention of nephrolithiasis. MEN'S HEALTH. 2009; 1: 154-156. |
| [22] | Borisov VV, Gordovskaya NB, Shilov EM. Phytotherapy with kanefron in nephrological practice: present and prospects (clinical lecture). CLINICAL NEPHROLOGY. 2010; 6: 39-42. |
| [23] | Areshidze DA, Mischenko DV, Makartseva LA, Kucher SA, Kozlova MA, Timchenko LD, Rzhepakovsky IV, Nagdalian AA, Pushkin SV. Some functional measures of the organism of rats at heart disease in two different ways. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML