D. A. Musakhodjaeva1, F. N. Nuraliev2
1Institute of Human Immunology and Genomics, Academy of Sciences of the Republic of Uzbekistan
2Urgench Branch of the Tashkent Medical Academy, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Urogenital candidiasis is widespread among women of reproductive age. The article provides immunological aspects of women of fertile age diagnosed with urogenital candidiasis (yeast fungi whose causative agents belong to the genus Candida - Candida albicans and Non albicans). The differentiation of various laboratory methods in the diagnosis of urogenital candidiasis requires a new approach to methods of identification, and, along with direct mycological methods, the development of indirect, accessible, inexpensive and highly effective diagnostic methods is important.
Keywords:
Urogenital candidiasis, Immunoglobulin, Humoral immunity, Cytokine status, Candida spp, Inflammation
Cite this paper: D. A. Musakhodjaeva, F. N. Nuraliev, Characterization of Immunological Aspects of Urogenital Candidiasis in Women of Fertile Age, American Journal of Medicine and Medical Sciences, Vol. 13 No. 2, 2023, pp. 63-66. doi: 10.5923/j.ajmms.20231302.07.
1. Introduction
The development of clinical immunology has been of great importance for understanding the pathogenesis of various infectious and noninfectious diseases. On the other hand, knowledge of the pathogenesis of the disease ensures its early diagnosis and timely treatment, increasing medical, social and economic efficiency. Based on the above, it is important to study the immunological aspects of each nosological unit. Urogenital candidiasis is a widespread disease that can occur in both sexes, but most often affects women of reproductive age [4]. Candida albicans is both a commensal and an opportunistic human fungal pathogen whose delicate balance is maintained by the actions of the innate immune system and the resident microbiota [1,6].To date, in various nosological units, the impact of the body's cellular immunity on quantitative and qualitative indicators, adequacy, specificity of changes in them has been studied, but the levels of changes in humoral immunity and cytokine concentrations have not been fully determined and are waiting to be addressed.The aim of the study was to investigate the immunological aspects of urogenital candidiasis in women of fertile age.
2. Material and Methods
A total of 135 women aged 19-59 with urogenital candidiasis participated in the study, 73 of whom were permanent residents of Khorezm region and 62 from Bukhara region. For this purpose, blood serum was taken from women of fertile age (15-49 years old) in whom the diagnosis of urogenital candidiasis was verified and the parameters of humoral immunity and cytokine status were evaluated. Modern clinical, instrumental, immunological, laboratory and statistical methods were used to perform this work.
3. Results and Discussion
Taking into account the composition of the vaginal microbiocenosis, the patients studied were divided into 3 groups (Elinov N.P., 2000):Group 1 - 22 women of fertile age with true candidiasis. Candida spp was a single pathogen, with more than 1x104 CFU/ml, quantitative and qualitative disturbance of normal vaginal microflora (dysbacteriosis) was not observed;Group 2 - 38 women of fertile age diagnosed with urogenital candidiasis in combination with vaginal dysbacteriosis. In this case Candida spp is cultured in association with Gram-positive cocci and Gram-negative bacteria belonging to pathogenic and conditionally pathogenic microorganisms (СPM). Candida spp at least 1x104 CFU/ml, pathogenic and UPM at least 1x109 CFU/ml were determined. It should be noted that in this case a quantitative and qualitative violation of the normal vaginal microflora (dysbacteriosis) was detected.Group 3 (control group) - 20 healthy women of fertile age with no history of urogenital candidiasis.To facilitate a comparative analysis of the results obtained, the overall rates of urogenital candidiasis compared with the control group were given. The results showed that the concentration of the studied immunoglobulins in the blood serum was significantly higher in the main group compared to the control group (Table 1).Table 1. Indicators of immunoglobulin concentrations in the serum of women diagnosed with urogenital candidiasis
 |
| |
|
In particular, we found that the level of IgA was 1.30 times significantly higher in the patient group compared to controls - 1.22±0.07 g/l versus 1.58±0.09 g/l, respectively (P<0.05). If we consider that IgA makes up 15% of all immunoglobulins, when a pathogen (infectious agent) enters the body, it is involved in the primary and secondary immune response against it, given its primary place in providing local immunity, which can justify the quantitative increase. High serum IgA levels ensure that mucosal surface production is high. Obtaining this immunoglobulin is a sign of activation of the body's immune system, including local immune factors.The patients' serum IgM concentration also increased in the main group, 1.02±0.07 g/l (up to 1.15 times) versus 1.17±0.08 g/l, respectively (P˂0.05). Given that IgM is produced first among immunoglobulins against foreign agents entering the bloodstream, this can be seen as an immunological sign that the infection has recently begun (Fig. 1).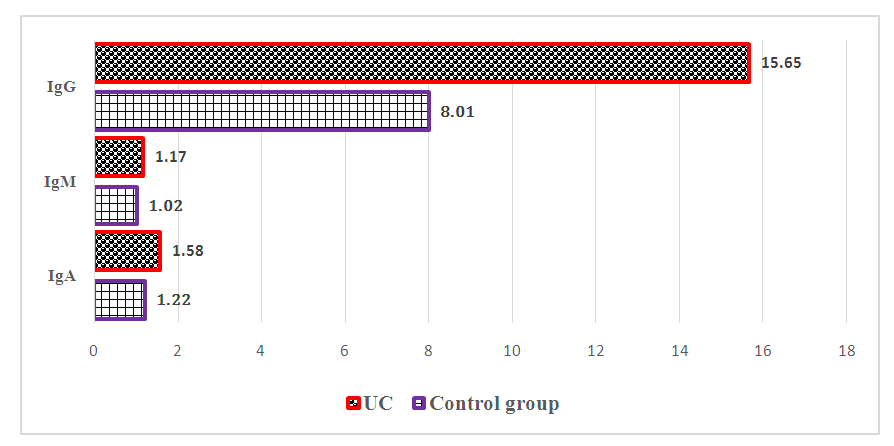 | Figure 1. Comparative parameters of the number of immunoglobulins in the blood serum of women with urogenital candidiasis, g/l |
IgG, which makes up 75% of immunoglobulins, mainly provides a secondary immune response and is produced after IgM, so the role of this immunoglobulin is huge in determining the prospect of ending the infection process. In our case, IgG was convincingly different (P<0.001) by a factor of 1.95 compared with the parameters of the control group in women who had verified urogenital candidiasis, 8.01±0.21 g/L versus 15.65±0.23 g/L, respectively (Figure 2).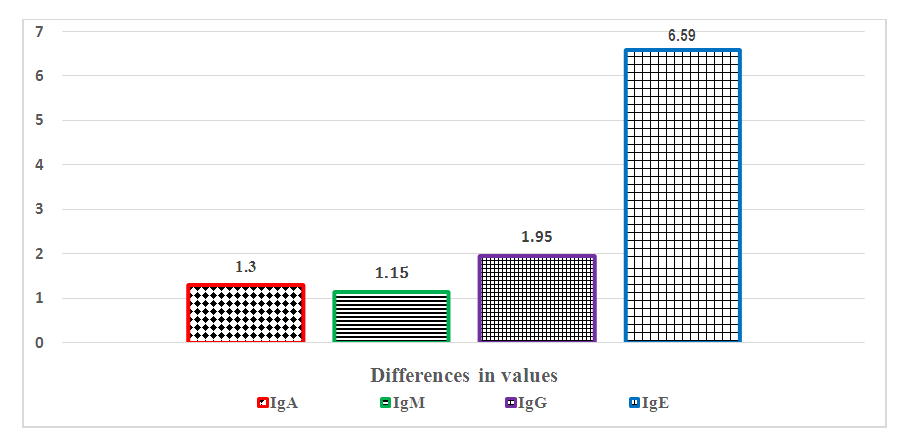 | Figure 2. Comparative serum immunoglobulin levels in women with urogenital candidiasis, how many times |
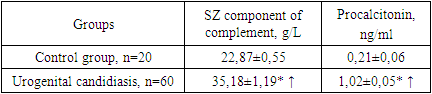
Increased concentration of immunoglobulins of all three classes in the blood serum indicates the presence of an inflammatory process in the body, that the causative agents of this process are of microbial nature. If you consider that the study did not identify a pathogen other than Candida spp, the cause of immunoglobulin hyperproduction becomes obvious.It has been proved that IgE in blood serum, unlike other immunoglobulins, is found in mammals, provides an individual immune response to an antigen (pathogen) that enters the body, has a certain biological activity (allergy), is not involved in primary and secondary immune responses as other immunoglobulins, is characterized by very low content in blood serum (0.2% of all immunoglobulins). Clinical trials denied the presence of atopic disease in all women studied, given the presence of a hereditary predisposition to IgE synthesis. The presence of parasitic infections in the body has also been disproved on the basis of clinical and parasitic studies, given that in most cases IgE is also elevated in parasitic diseases. These clinical and parasitic studies ensured the purity of the clinical and immunological study performed.The results showed that the amount of IgE in the patients' serum was 6.59 times that of the control group, 24.46±1.05 g/L versus 161.19±7.1 g/L, respectively (P<0.001). Apparently, urogenital candidiasis was accompanied by a strong allergic background.A tendency toward an increase in the concentrations of immunoglobulins, which provide the primary and secondary immune response in the body, was also observed in the amounts of the SZ-component of complement and procalcitonin, which are nonspecific protective agents (Table 2).Table 2. Parameters of nonspecific protective factors in the serum of women diagnosed with urogenital candidiasis
 |
| |
|
The concentration of serum complement component SZ tended to decrease in patients, 22.87±0.55 g/L versus 35.18±1.19 g/L, respectively (to 1.54 times, Р<0,001).C3 component of complement is an important component of complement, is part of the proteins of the acute phase of inflammation, the process of phagocytosis, the systemic inflammatory process occurring in the body is enhanced by opsonization of pathogens that have entered the body. Consequently, an increase in the C3 component of complement provides not only an increase in nonspecific factors of the immune system, but also increases the process of phagocytosis.Procalcitonin was identified as one of the indicators of systemic inflammatory process occurring in the body, if we take into account that it multiplies during bacterial infection, has high specificity and sensitivity to other inflammatory markers (C-reactive protein, leukocytosis, etc.), it becomes clear that we chose it for detection. While procalcitonin was detected in the control group at an average of 0,21±0,06 ng/mL, in female patients it averaged 1,02±0,05 ng/mL. Результат оказался статистически значимым, при этом разница между результатами составила 4,86 раза (Р<0,001).It is known that cytokines are molecules of small peptide nature that are highly informative, transferring information between specific and nonspecific cells of the immune system, ensuring primary and secondary immune response, as well as controlling it. Quantitative changes in inflammatory and anti-inflammatory cytokines indicate the extent of the inflammatory process, pre-tumor and pathological conditions in the body. Among the anti-inflammatory cytokines that differentiate this pathological process, we found it necessary to define interleukin-4 (IL-4), which induces the differentiation of Th0 cells (initial T-helper cells) into Th2 cells, which is important for the completion of the immune response, also one of the cytokines involved in inflammation, tumor necrosis factor-α -TNF-α. The reason for choosing TNF-α is that it is one of the mediators of the inflammatory process and provides an immune response.The results showed that in the control group, IL-4 and TNF-α, while being within the limits of the accepted norm or reference values, showed close results to those of the control group - 4.52±0.25 ng/ml and 4.11±0.08 ng/ml, respectively (Table 3).Table 3. Indicators of serum cytokine status in women diagnosed with urogenital candidiasis
 |
| |
|
In women with urogenital candidiasis, these parameters showed a convincing increase in serum (P<0.001). Whereas there was a 2.46-fold increase in IL-4 in healthy women of the control group compared with those in the control group (to an average of 11.12±0.71 ng/ml). TNF-α cytokinin values manifested multiple increases, up to 11.12±0.71-fold (mean to 46.31±1.59 ng/mL), P<0.001.It is noteworthy that statistically significant differences in the numbers are equal to the increase in both cytokines. Separately, we should note that proinflammatory cytokine (TNF-α) concentrations exceeded those of proinflammatory cytokine (IL-4) in terms of prevalence. This condition can also be seen when their ratio to one is observed - 11.12: 4.52 = 2.46 and 46.31: 4.11 = 11.27 (Fig. 3).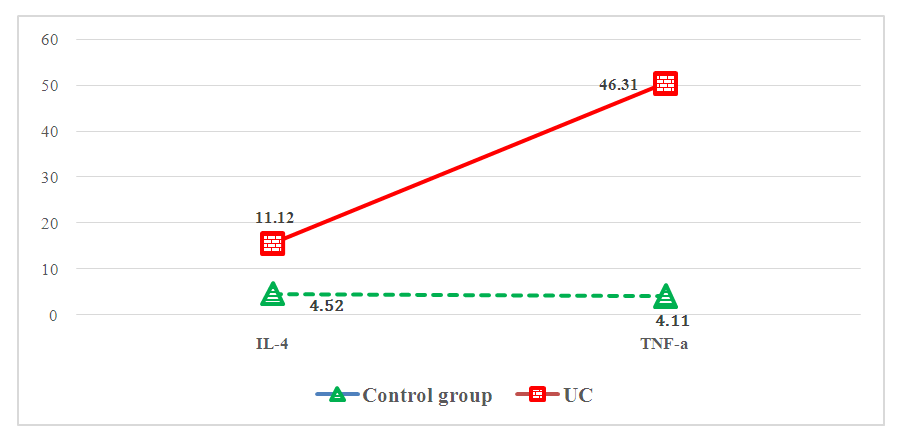 | Figure 3. Indicators of serum cytokine status in women with urogenital candidiasis, ng/ml |
In our opinion, the concentration of cytokines in the blood serum, which cause inflammation and are directed against it, changes according to the end of the disease, the course of the inflammatory process occurring in the body, when the concentration of one of them prevails over the other, then the result indicates the course of the inflammatory process. The fact that TNF-α, which in our case supports inflammation, is quantifiable in relation to the anti-inflammatory IL-4, indicates a clear development of this pathological condition. Consequently, it has been proven that inflammation developed strongly at the stage of obtaining biological material from patients. This proven law serves for early diagnosis of the disease at the time of determining the level of development of urogenital candidiasis, perspective and its cessation.Considering the above, anti-inflammatory cytokine IL-4 and proinflammatory cytokine TNF-α are recommended as additional diagnostic and prognostic immunological criteria.
4. Conclusions
1. Patients with urogenital candidiasis had IgA 1.30 times (P<0.001), IgM 1.15 times (P<0.05), IgG 1.95 times (P<0.001), and IgE 6.59 times (P<0.001) higher than the control group. The increased amount of IgA, IgM and IgG was explained by an increase in the overall local immune activity in relation to the infectious agent by strengthening the primary and secondary immune response, while the increase in IgE was explained by the presence of this disease against a strong allergic background. 2. It has been established that in women with urogenital candidiasis, the concentration of the SZ Component of complement and procalcitonin from nonspecific factors of the body's immune system were significantly higher than in healthy individuals - up to 1,54 and 4,86 times, respectively (P<0.001). These indicators, which provide humoral immunity, were properly corrected with an increase in the concentration of immunoglobulins. This circumstance made it possible to determine the degree of development of the inflammatory process.
References
| [1] | Bojang, E.; Ghuman, H.; Kumwenda, P.; Hall, R.A. Immune Sensing of Candida albicans. J. Fungi 2021, 7, 119. https://doi.org/10.3390/jof7020119. |
| [2] | Zarochentseva N.V., Belaya Yu.M. The problem of urogenital candidiasis in women in the modern world // BC. 2016. No. 15. P. 976–981. The original article was published on the RMJ website (Russian Medical Journal): http://www.rmj.ru/articles/ginekologiya/Problema_urogenitalynogo_kandidoza_u_ghenschin_v_ sovremennom_mire/#ixzz7rBoeKTpT. |
| [3] | Nuraliev N.A., Bobojonov H.R., Nurmetov F.E. Indicators of morbidity of urogenital candidiasis // Nazariy va klinik tibbiyot jurnali. - Tashkent, 2010. - №6. - P.79-82. |
| [4] | Savicheva A.M., Shipitsyna E.V., Recurrent urogenital candidiasis: peculiarities of diagnosis and treatment // Medical Advice. 2015. №9. P. 15-17 Tikhomirova EV, Balan VE, Ovchinnikova VV. Modern views on the treatment of recurrent urogenital candidiasis. Russian Bulletin of Obstetrician-Gynecologist. 2020; 20(5): 116 120. (In Russ.). https://doi.org/10.17116/rosakush202020051116. |
| [5] | Ward, T.L.; Knights, D.; Gale, C.A. Infant fungal communities: Current knowledge and research opportunities. BMC Med. 2017, 15, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version] |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML