-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(2): 60-62
doi:10.5923/j.ajmms.20231302.06
Received: Jan. 16, 2023; Accepted: Feb. 9, 2023; Published: Feb. 13, 2023

Peculiarities of Clinical Course and Diagnostics of Castration-Resistant Prostate Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTillyashaykhov Mirzagolib Nigmatovich1, Iskandarov Jakhongir Mashrabjon Ugli2, Boltaev Mashrab Iskandarovich2, Boyko Elena Vladimirovna3, Nodir Makhamatkulovich Rahimov4
1Doctor of Medical Sciences, Professor Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
2Bukhara Branch of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
3Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
4Doctor of Medical Sciences, Samarkand State Medical University, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of this article was to study the peculiarities of clinical course and diagnostics of primary castration-resistant prostate cancer. The study was based on the data analysis of 112 patients with hormone-resistant prostate cancer (HRPC) under observation at the oncourology department of the RSNPMCRC from 2008 till 2021, of which 20,5% patients had primary resistance to hormonal therapy. Symptoms and signs of urinary tract obstruction, such as difficulty urinating, increased urinary frequency, and a feeling of incomplete emptying, were present in most of our patients. Chronic retention and bilateral hydronephrosis with renal insufficiency were observed in 3 patients. Two patients had urinary incontinence due to sphincter infiltration. All possible, routine means of imaging and histological examination of the tumor should be used to determine the development of hormonal resistance of BPH.
Keywords: Castration-resistant cancer, Prostate gland, Hormonal resistance, Histological study
Cite this paper: Tillyashaykhov Mirzagolib Nigmatovich, Iskandarov Jakhongir Mashrabjon Ugli, Boltaev Mashrab Iskandarovich, Boyko Elena Vladimirovna, Nodir Makhamatkulovich Rahimov, Peculiarities of Clinical Course and Diagnostics of Castration-Resistant Prostate Cancer, American Journal of Medicine and Medical Sciences, Vol. 13 No. 2, 2023, pp. 60-62. doi: 10.5923/j.ajmms.20231302.06.
1. Introduction
- According to the data of Tillashayhov et al. (2021) prostate cancer (BC) makes up 10,0% of malignant neoplasms in general population in the territory of the Republic of Uzbekistan [1,2,7,8]. The variability of the clinical picture of BPH, as well as the frequently occurring asymptomatic course of the disease up to generalization of the process make an early diagnosis of the appearance of resistant BPH difficult [3,5]. The first step in determining hormonal resistance is the fact that conventional methods of hormonal therapy for BPH are unsuccessful. Hormonal resistance of the tumor in some patients with PCa is determined immediately after the start of treatment, in others it develops after several months of successful treatment with hormonal therapy[4,6]. Despite this, to date, there are no characteristic signs and reliable criteria for determining the primary and secondary forms of hormonal resistance, which complicates the choice of adequate therapy for each patient with BPH [9].
2. Materials and Methods
- Our study was based on data analysis of 112 patients with hormone-resistant prostate cancer (HRPC) under observation in the oncourological department of the RSNPMCRC from 2008 to 2022.
3. Results
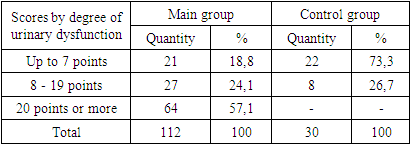
- Symptoms and signs of urinary tract obstruction, such as difficult urination, increased frequency of urination and feeling of incomplete emptying, were present in most of our patients. Chronic retention and bilateral hydronephrosis with renal insufficiency were observed in 3 patients. Two patients had urinary incontinence due to sphincter infiltration. Unfortunately, in most patients the first symptoms were moderate pelvic pain and sometimes lumbar pain, which is the result of tumor progression. One patient had recurrent thrombophlebitis, disseminated intravascular coagulation and bleeding, due to intense bone marrow involvement. In one patient, subclavian adenopathy was the first manifestation of the disease. The clinical diagnosis of hormone-resistant PCa was established in case of increasing PSA level and/or objective appearance and/or progression of metastases against the background of castrated blood testosterone level. The criteria for this condition were as follows: - Castration blood testosterone levels (< 50 ng/mL); - an increase in PSA demonstrated in three consecutive tests performed at least 2 weeks apart, or - appearance and progression of bone or soft tissue metastases. There are many works devoted to diagnosis of probable progression of PCa, including occurrence of hormone-resistant forms, by one or other methods of investigation. All patients of the main and control groups were assessed for the degree of urinary dysfunction according to IPSS (Table 1).
|
|
|
4. Conclusions
- To date, there is no specific time frame for concluding tumor resistance to hormone therapy after unsuccessful hormone therapy. All possible, routine imaging and histological examinations of the tumor should be used to determine if hormonal resistance has developed.