Sarvinoz Khaydarova, Shakar Navruzova
Department of Pediatrics, Bukhara State Medical Institute, Bukhara, Republic of Uzbekistan
Correspondence to: Sarvinoz Khaydarova, Department of Pediatrics, Bukhara State Medical Institute, Bukhara, Republic of Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article is devoted to the study of the parameters of the immune system in atypical angina in men and women, the authors evaluated the cytokine status depending on gender, which is of great importance for health authorities in the organization of specialized cardiological and therapeutic services. The proposed method allows early diagnosis and prevention of the development of atypical angina, which is of great practical importance.
Keywords:
Atypical angina pectoris, Ischemic heart disease, Men, Women, Cytokines
Cite this paper: Sarvinoz Khaydarova, Shakar Navruzova, Gender Features of Cytokine Status in Atypical Angina, American Journal of Medicine and Medical Sciences, Vol. 13 No. 2, 2023, pp. 47-50. doi: 10.5923/j.ajmms.20231302.03.
1. Introduction
The most important problem of modern healthcare is coronary heart disease (CHD), which is characterized in the WHO materials as an epidemic of the present time and one of the leading causes of mortality. In the clinical manifestation, coronary heart disease may debut acutely – as a myocardial infarction (MI) or sudden coronary death, or develop gradually, having periods of stable course and exacerbation. Periods of exacerbation are designated by the term acute coronary syndrome (ACS), which combines two clinical conditions – unstable angina and myocardial infarction. The concept of ACS includes any clinical signs or symptoms that make it possible to suspect acute myocardial infarction (AMI) or unstable angina [1,2,3,6]. The most typical complaint of patients with stable angina is a feeling of discomfort or chest pain of a compressive, pressing nature, which is localized most often behind the sternum and can radiate to the left arm, neck, and lower jaw. However, some patients may have angina atypically. Thus, cases of localization of pain syndrome in the right half of the chest, in the rectum, in the first toe when walking, and even acute toothache are described [4,5,7]. The data presented mainly in foreign literature indicate the insufficient commitment of women to physical training and their lower motivation to participate in rehabilitation programs compared to men. Foreign scientists provide data that men and women have different effects from ongoing rehabilitation measures, even with their comparable age, height and muscle mass. It was also found that women are more likely to have lower physical activity both before and after the onset of ACS [8-12]. The study of the influence of gender differences on the prognosis and course of cardiovascular diseases remains relevant. Some domestic and foreign scientists have studied the features of clinical manifestations and treatment of cardiovascular diseases in men and women. It was determined that women are more likely to have a more severe course of coronary heart disease (CHD) than men and a greater number of risk factors. However, there is little data in the literature concerning the study of protein growth factors and damage in patients with arterial hypertension, taking into account gender [1]. The study aims to study the cytokine status in atypical angina, depending on gender, to develop early markers of atypical angina.
2. Materials and Methods
The study included 104 patients with atypical angina (AA) aged 47 to 85 years (the average age of men was 67.8 ± 9.8 years, and women 68.0 ± 8.6 years). The comparison group consisted of patients with ischemic heart disease (CHD) with arrhythmia. A total of 60 patients, including 30 women (average age 66.5 ± 8.5 years) and 30 men (average age 65.4 ± 8.4 years). AA verification was carried out according to the requirements of the World Health Organization (WHO), classified according to the International Classification of Diseases (ICD-10).The content of cytokines (IL-1, IL-6, IL-10, TNF-α) in blood serum was studied by enzyme immunoassay using the "Vector-Best" test systems with a set of reagents A-8768, Russian Federation, Novosibirsk.The exclusion criteria from the study were acute myocardial infarction, type 1 diabetes mellitus, unstable angina pectoris, pheochromocytoma, atrial fibrillation, acute cerebrovascular accident, dyscirculatory encephalopathy, urolithiasis, cholelithiasis, bronchial asthma, сhronic pulmonary obstructive disease (COPD).
3. Results and Discussion
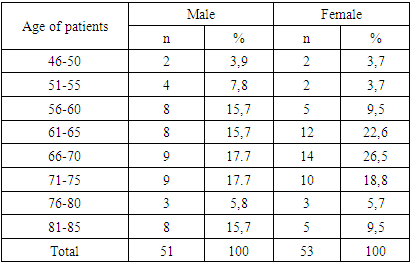
The ratio of males-51 (49.0%) and females-53 (51.0%) was 1:1.03.The study of bad habits in men with AA was of interest, it was found that among all the surveyed men, the number of non-smokers was higher - 38 (74.5%) than smokers - 13 (25.5%). The gender distribution of patients with AA showed an increase in cases of AA in women aged 61 to 75 years - 36 (67.9%) and in men aged 56 to 85 years - 45 (88.3%) (Table 1).Table 1. Distribution of patients with AA by gender and age
 |
| |
|
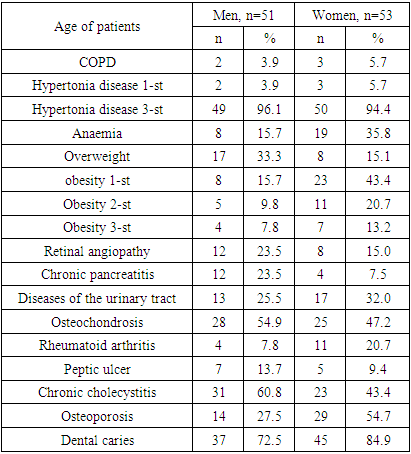
An important element of the study is the study of gender characteristics of the mechanism of AA development, which requires a comprehensive study of hormonal status, the state of carbohydrate metabolism, and lipids in the blood.In the course of studying the peculiarities of the course of AA, depending on gender, very interesting facts were obtained indicating the relationship of the mechanism of AA development with existing metabolic disorders of other substances in the body. In particular, the relationship with hormonal, biochemical and cytokine status. Eventually, syntropia was established in AA, that is, every patient with AA has concomitant diseases.Depending on the gender and severity of AA, an analysis of the state of comorbidity was performed and revealed the predominance of hypertension in the structure of comorbidity in AA, regardless of gender (Table 2).Table 2. The frequency of syntropia in AA in the examined patients
 |
| |
|
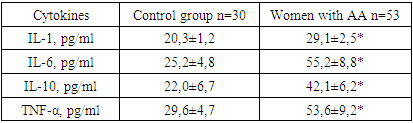
In all patients with AA of varying severity, the course was established. At the same time, among all patients, grade 1 hypertension is noted in 5 patients (4.8%), and in other cases, grade 3 hypertension is 99 (95.2%), which acts as an aggressive factor in the development of AA in both men and women.AA is characterized by a comorbid course. The information obtained shows the importance of taking into account the gender characteristics of the formation and course of AA, depending on age.The analysis of the nosological structure of AA comorbidity showed the predominance of hypertension regardless of gender. Dental caries occupies the second place of comorbidity, which is 37 (72.5%) in men, and 45 (84.9%) cases in women. The third place in men is occupied by chronic cholecystitis-31 (60.8%), and in women - osteoporosis of bones-29 (54.7%).Thus, the obtained research data showed the importance of taking into account the comorbid state in patients with AA for timely early prevention of complications and prediction of the course of the underlying disease. The fact of presence of comorbidity proves the complexity of the mechanism of AA development, especially in middle-aged people. Therefore, it is very important to study cytokines in AA to optimize the management tactics of patients in this category.Pro- and anti-inflammatory cytokines are considered important mediators of intercellular interactions in the immune system, as well as the main mediators of neuroimmune interactions. The study of cytokines in women with AA showed an increase in the level of IL-1 to 29.1±2.5 pg/ml in relation to the indicators of patients of the comparative group - 20.3±1.2 pg/ml, P<0.05 (Table 3).Table 3. Cytokines in atypical angina in women
 |
| |
|
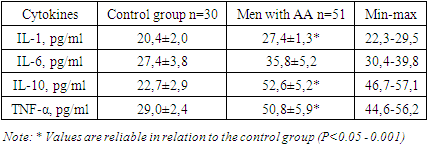
At the same time, the threshold level indicating the development of inflammation in AA in women is the concentration of IL-1 >25.4 pg/ml. AA in women is also accompanied by an increase in the level of IL-6 by 2.2 times (-55.2±8.8 pg/ml), against the values of the comparative group -25.2±4.8 pg/ml.Taking into account the above data, a study was conducted to determine the level of IL-10 in the blood of the examined patients. As a result, its concentration increased by 1.92 times in AA in women up to 42.1±6.2 pg/ml against the values of the comparative group - 22.0±6.7 pg/ml. Consequently, the results obtained confirm the process of violation of microcirculation in the myocardium and activation of protection. At the same time, an increase in the concentration of TNF-α in the blood was revealed to -53.6±9.2 pg/ml in relation to the indicators of the comparison group-29.6±4.7 pg/ml. Consequently, in women with AA, in response to damage to the vascular wall as a result of impaired microcirculation in the myocardium and spasm of coronary vessels, there is a tendency to increase TNF-α in the blood. Thus, the mechanism of AA development in women is closely interrelated with the violation of intercellular interaction at the level of cellular structures, which is determined by the state of synthesis of pro and anti-inflammatory cytokines. The activity of inflammatory markers has an important prognostic value for assessing the progression of CVD. Postmenopausal women have a high risk of developing and progressing CVD. For early detection of the risk of developing AA and the prevention of coronary heart disease in women, it is important to regularly examine and study the cytokine status. Studying the gender characteristics of risk factors for the development of AA, we did not find data on the implementation of cytokine synthesis depending on gender.The pathomechanism of the course of AA in men at the molecular level was interesting. For a comparative evaluation of the data obtained, studies were conducted to study the cytokine profile. A significant increase in the concentration of IL-1 in men was revealed -27.4±1.3 pg/ml against the values of the comparison group-20.4±2.0 pg/ml (p<0.05). The obtained result proves the presence of systemic inflammation in AA in men (Table 4).Table 4. Cytokines in atypical angina in men
 |
| |
|
IL-6 in AA in men tends to increase to 35.8±5.2 pg/ml, compared to the comparative group - 27.4±3.8 pg/ml.Taking into account the data of modern research by scientists of the world proving that IL-6 is a neurocytokine, the results of our studies in men with AA confirm the involvement of brain vessels in the process with the risk of developing cerebral complications.To predict the development of AA complications and the state of the body's defence at the cellular level, we also studied the concentration of IL-10, which allowed us to establish its increase by 2.3 times in men, concerning the indicators of the comparative group -22.7± 2.9 pg/ml.Consequently, the obtained result of studying IL-10 in AA in men shows the importance of compensatory defence mechanisms aimed at preserving coronary and cerebral microcirculation.The indicator of cell death and tissue apoptosis with subsequent decay and the risk of transformation of ACS into MI and /or angina indicate the outcome and severity of the course of AA. The study found a statistically significant increase in the level of TNF-α by 1.75 times (up to 50.8±5.9 pg/ml) in relation to the indicators of the comparative group-29.0±2.4 pg/ml. Thus, the cytokine status in men with AA is aimed at preserving the compensatory mechanisms of the body's defence to improve coronary and cerebral circulation. Taking into account the above, the established research data allowed for predicting the outcome of AA and determining informative indicators of the development of complications, taking into account gender. At the same time, for women, the threshold level indicating the development of inflammation in AA is the concentration of IL-1 >25.4 pg/ml. Indicators of the severity of the course of AA are anaemia, uremia and an increase in the atherogenicity index > 2.5 Conv. units. For men, the concentration of IL-1>27.4 pg/ml is indicative of the development of inflammation in AA. Indicators of the severity of AA in men are the state of prediabetes (hyperglycemia, hypertriglyceridemia).
4. Conclusions
1. Syntropia in AA has been established, and regardless of gender, hypertension prevails in the structure of comorbidity. The second place of comorbidity is occupied by dental caries, which is 72.5% in men and 84.9% in women, the third place in men is occupied by chronic cholecystitis-60.8%, and in women - osteoporosis of bones-54.7%.2. For women, the threshold level indicating the development of inflammation in AA is the concentration of IL-1 >25.4 pg/ml. Indicators of the severity of the course of AA are anaemia, uremia and an increase in the atherogenicity index > 2.5 Conv. units.3. For men, the concentration of IL-1>27.4 pg/ml is indicative of the development of inflammation in AA. Indicators of the severity of AA in men are the state of prediabetes (hyperglycemia, hypertriglyceridemia). With AA, a comprehensive study of the cytokine status, the state of carbohydrate metabolism, and lipids in the blood are necessary. For the prevention of coronary heart disease and for early detection of the risk of developing CVD, regular examination and study of blood cytokines (IL-1, IL-6, IL-10 and TNF-α) are necessary, for the prevention of cerebral complications of AA, a study of IL-6 in dynamics is recommended.
ACKNOWLEDGEMENTS
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to the authors/ editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.The Source of funding is nil.
References
| [1] | Абзалиев, К.Б., Алдангарова, Г.А., Абзалиева, С.А., Актаева, Л.М., Мусабекова, Ж.Б. and Насырова, Н., 2019. Состояние вопроса гендерных различий при заболеваниях сердца и факторы риска. Наука о жизни и здоровье, (1), pp.49-58. doi:10.24411/1995-5871-2019-10005. |
| [2] | Бубнова, М.Г., Новикова, Н.К., Аронов, Д.М., Красницкий, В.Б. and Кадушина, Е.Б., 2016. Клиническое 16-летнее наблюдение за больными, перенесшими острый инфаркт миокарда: феномен высокой приверженности к физической реабилитации. Вестник восстановительной медицины, (4), pp.12-19. |
| [3] | Ганиева, Ш.Ш. and Яхъяева, Ф.О., 2022. Современные патогенетические аспекты кардиоренального синдрома. Eurasian Journal of Medical and Natural Sciences, 2(6), pp.167-173. |
| [4] | Линчак, Р.М., Догадова, Т.В. and Жирова, Л.Г., 2011. Атипичная стенокардия: особенности диагностики и лечения. Вестник Национального медико-хирургического центра им. НИ Пирогова, 6(4), pp.135-136. |
| [5] | Наврузова, Ш.И., 2022. Диагностическое Значение Показателей Клеточного Иммунитета При Артериальной Гипертензии. Central Asian journal of medical and natural sciences, 3(2), pp.421-426. doi: 10.17605/OSF.IO/4FXQ9. |
| [6] | Хороших, О.А., 2013. Атипичные варианты инфаркта миокарда. Клинический случай редкой формы острого коронарного синдрома с периферическим эквивалентом стенокардии. Acta Biomedica Scientifica, (5 (93)), pp.104-107. |
| [7] | Ganieva Sh.Sh, and Akhrorov, J.X., 2022. Этиопатогенетические Особенности Ремоделирования Сердца При Кардиоваскулярной Патологии. Periodica Journal of Modern Philosophy, Social Sciences and Humanities, 13, pp.101-105. |
| [8] | Minges, K.E., Strait, K.M., Owen, N., Dunstan, D.W., Camhi, S.M., Lichtman, J., Geda, M., Dreyer, R.P., Bueno, H., Beltrame, J.F. and Curtis, J.P., 2017. Gender differences in physical activity following acute myocardial infarction in adults: a prospective, observational study. European journal of preventive cardiology, 24(2), pp.192-203. doi: 10.1177/2047487316679905. |
| [9] | Kim, J.H., Kim, J.W., Ko, Y.H., Choi, C.U., Na, J.O., Kim, E.J., Rha, S.W., Park, C.G., Seo, H.S. and Oh, D.J., 2010. Coronary endothelial dysfunction associated with a depressive mood in patients with atypical angina but angiographically normal coronary artery. International journal of cardiology, 143(2), pp.154-157. doi: 10.1016/j.ijcard.2009.02.004. |
| [10] | Poorna T, A., Ek, J. and John, B., 2022. Ludwig's angina in a COVID-positive patient—An atypical case report. Special Care in Dentistry, 42(1), pp.99-102. doi: 10.1111/scd.12643. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML