Mukhtarov Shukhrat Tursunovich1, Nasirov Furkat Raupovich2, Kayumov Abdurauf Abdumavlyanovich3
1Administration, Republican Specialized Scientific-Practical Medical Center of Urology MoH RUz, Tashkent, Uzbekistan
2Department of Science, Republican Specialized Scientific-Practical Medical Center of Urology MoH RUz, Tashkent, Uzbekistan
3Clinic Department, Republican Specialized Scientific-Practical Medical Center of Urology MoH RUz, Tashkent, Uzbekistan
Correspondence to: Kayumov Abdurauf Abdumavlyanovich, Clinic Department, Republican Specialized Scientific-Practical Medical Center of Urology MoH RUz, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The aim of the study was to evaluate the effectiveness, safety and advantages of the introduction of modern endoscopic methods for the removal of coralloid stones (CC) in a comparative aspect with traditional methods. Prognostic efficacy of additional procedures was also evaluated: extracorporeal (remote) shock wave lithotripsy (EShWL) and percutaneous nephrolithotripsy (lithotomy) (PCNLT). After endoscopic access using such additional methods as EShWL and PCNLT the rate of detection was on the average 8,2%, and after conventional surgical intervention it was statistically significantly more frequent - 31,8% of cases (p<0,001). Our study has shown a significantly greater efficacy, reduction of the frequency and severity of adverse events and improvement of prognostic indicators achieved by using endoscopic method, in comparison with the traditional open access surgical intervention.
Keywords:
Corral stones (CC), Extracorporeal (remote) shock wave lithotripsy (EShWL), Percutaneous nephrolithotripsy (lithotomy) (PCNLT), Endoscopic method, The traditional open access surgical intervention
Cite this paper: Mukhtarov Shukhrat Tursunovich, Nasirov Furkat Raupovich, Kayumov Abdurauf Abdumavlyanovich, Peculiarities of Percutaneous Surgery for Coral Calculi, American Journal of Medicine and Medical Sciences, Vol. 13 No. 1, 2023, pp. 6-9. doi: 10.5923/j.ajmms.20231301.02.
1. Introduction
The incidence of urolithiasis, according to the data of appealability, is 200–245 per 100,000 population. The true incidence of urolithiasis in the population, detected during preventive examinations, is 3–3.5 times higher [1].In different regions of the world, the incidence varies from 5-9% in Europe, to 1-5% in Asia and up to 20% in North America [2].In urological hospitals, patients with urolithiasis (UCD) account for up to 40% of the total contingent. In 35-75% of them, the disease is recurrent. Surgical interventions for UCD in 25% lead to various complications and in 11% end with nephrectomy, in 3% - with a lethal outcome [3,4,5].The history of percutaneous kidney surgery in the Republic of Uzbekistan has about 44 years. Thus, the first nephrostomy under X-ray control was performed in 1978. (Department of Urology of Tashkent Institute of Medical Education (TIPME), professor Mukhtarov O.M.), and the first nephrolithoextraction was performed – 1987. (Department of Urology and Operative Nephrology, TashGosMi, Prof. Arustamov D.L.).The development of modern technologies makes it possible to introduce modern, high-tech methods into the practice of modern urology [6-11].
2. Purpose of the Study
To evaluate the effectiveness of the introduction of modern endoscopic methods for the removal of CC in a comparative aspect with traditional methods.
3. Materials and Methods
The results of treatment of 226 patients with coral and multiple kidney stones were retrospectively studied (K3). The studied patients could be subdivided into subgroups according to the method of surgical intervention used. Thus. 100 patients (48.6%) underwent endoscopic method and 116 (51.4%) underwent traditional method. Distribution of patients of the study group by gender is shown in Figure 1.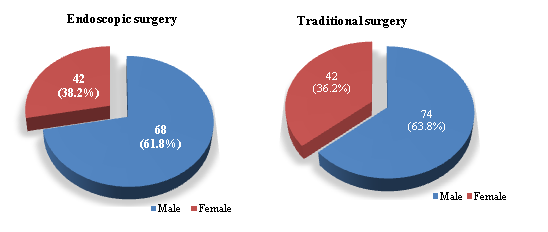 | Figure 1. The scheme of separation of patients according to the method of surgical intervention and by gender |
As is known, CCs are referred to complex stones. A simplified and convenient definition for CCs was used depending on the part of the calyx-lobule system (CLS) occupied: - Borderline (K1 - pelvis and any one calyx: less than 50.0% of the volume of the PSC);- Partial (K2 - pelvis and more than two calyces: 50.0-80.0% of the volume of the PNS);- Complete (K3 - entire CLS or more than 80.0% of its volume)The presence, size, and shape of the stones were verified using an instrumental method of examination: multislice computed tomography (MSCT) (Fig. 2).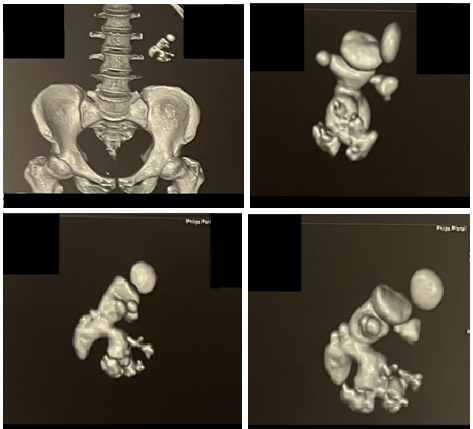 | Figure 2. Corral stone on multispiral 3D computed tomography |
Patients with CC were divided into the following groups:I-Group - underwent endoscopic intervention: ü The operations were performed under spinal muscular analgesia (SMA), in the position of the patient on the abdomen.ü Contact disintegration of the stone was carried out by ultrasound and combined method.ü The size of the nephroscope tube was 24-26 СН.II-Group - those who underwent conventional intervention: ü Lumbotomy under endotracheal anesthesia.Features of the technique:ü puncture on a stone;ü no discharge on the needle;ü boring to the distal part of the stone;ü disintegration and release of the cup to insert the nephroscope tube into the hls:ü using the tube as an ampullary shroud;ü performing a second access based on the localization of the residual stone;ü use of the "needle technique" to remove single stones.
4. Results
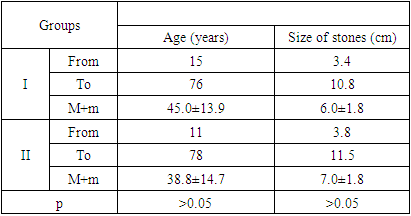
The study first analyzed the age structure of the study groups of patients with CK as presented in Table 1. In general, the groups were comparable in age and stone size, with no significant differences.Table 1. The ratio of stone size and age of patients
 |
| |
|
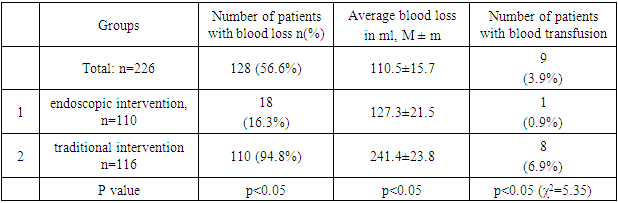
We compared the number of cases and volume of blood loss among patients who underwent the traditional method of surgical intervention and the innovative endoscopic method (Table 2). Thus it was found that the endoscopic method had 16.3% of patients with blood loss which was significantly - in 5.8 times (p<0.05) lower than the traditional method of investigation when the blood loss occurred in 94.8%. The average volume of blood loss at endoscopic method was 1.9 times less (p<0.05) than at traditional type of intervention. The number of patients who required blood transfusion using endoscopic method was 0.9%, which is 7.7 times lower (p<0.05) compared to the group of patients with traditional method of operation, where their proportion was 6.9%.Table 2. Frequency and volume of intraoperative blood loss
 |
| |
|
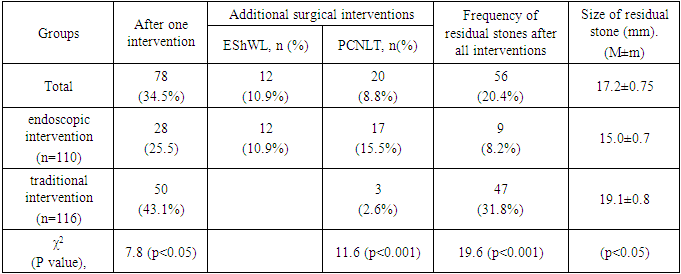
Differences in the quantity and quality of residual stones observed after the methods of surgical intervention compared in this study were also revealed. So, after a single endoscopic intervention, residual stones were observed in 25.5% of cases, which was statistically significant - 1.7 times lower (p<0.05) than after traditional surgery, in which the recurrence rate was observed in 43.1% cases.The prognostic effectiveness of additional procedures was also assessed: extracorporeal (remote) shock wave lithotripsy (EShWL) and percutaneous nephrolithotripsy (lithotomy) (PCNLT). Thus, the incidence of residual stones when using endoscopic access after EShWL was 10.9%, and after PCNLT - 15.5%. When using the traditional access of surgical intervention after the use of additional PCNLT, residual stones were detected in 2.6% of cases.Thus, in general, the formation of residual stones was observed in an average of 20.4% of cases. At the same time, after the use of endoscopic access using such additional methods as EShWL and PCNLT, the detection rate averaged 8.2%, and after the use of traditional surgery, it was statistically significantly more frequent in 31.8% of cases (p<0.001). Differences were also found in the size of residual stones. If after the use of endoscopic access their average size was 15.0±0.7, which was noticeable - 1.26 times less (p<0.05) than after the traditional intervention, where the size of residual stones averaged 19.1 ±0.8 (table 3).Table 3. Information about residual stones
 |
| |
|
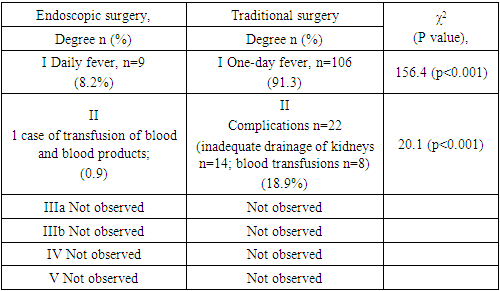
The observed postoperative complications presented in Table 4 were analyzed. The frequency of one-day fever during endoscopic intervention was observed in 8.2% of cases, which was significantly less than during traditional intervention - 91.3%. In addition, the use of the traditional type of intervention required additional prescription of antipyretic drugs. Also, when using the traditional method, hematuria through the nephrostome or during urination could be observed in 53.4% of cases; therefore, diuretics and hemostatics were additionally prescribed.While the endoscopic method required hemotransfusion only in one case, which was 0.9%, the traditional method required blood and blood products transfusion in 8 cases (6.9%). Besides, at a traditional method in 14 cases (12,1%) inadequate drainage of the kidneys with subfebrile temperature for more than 2 days was observed, which required correction of the antimicrobial therapy. On the whole, these complications with traditional methods of treatment required additional measures (hemotransfusions and correction of antimicrobial therapy) in 22 cases (18.9%). In grades IIIa, IIIb, IVa,b, and V, no complications were observed (Table 4).Table 4. Font Specifications for A4 Papers
 |
| |
|
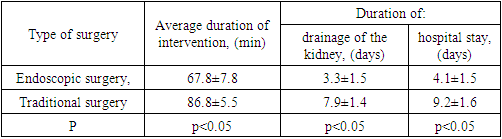
The causes of intraoperative complications, as a rule, were:ü incorrect choice of access to the stone;ü features of the configuration of stones;ü the duration of the intervention;ü anomaly of the kidney and blood vessels;ü damage to the neck of the calyx;Table 5. Intra- and postoperative indicators
 |
| |
|
When using endoscopic access the average duration of intervention was 1.28 times shorter (P<0.05) than when using traditional open access. Also when using endoscopic method of surgical intervention the time of kidney drainage was also reduced, which was 2.4 times shorter (p<0.05) than the traditional method. As it is known, the duration of surgical intervention directly influences the incidence of various postoperative complications and the shorter it is, the lower is the probability of their occurrence and severity of their manifestation. Also, the average time of hospital stay was more than halved from 9.2±1.6 when using traditional method to 4.1±1.5 when using endoscopic method.Thus, our study showed significantly greater efficacy, reduction in the frequency and severity of adverse events and improvement in prognostic indicators achieved when using endoscopic method, in comparison with the traditional open access surgical intervention.
5. Conclusions
Percutaneous nephrolithotripsy is the method of choice in the treatment of coral nephrolithiasis.The distal part of the stone outgrowth in the calyx is preferably disintegrated against the installed nephroscope tube at the level of the kidney parenchyma, followed by the release of the calyx, which allows to move the nephroscope tube into the calyx to disintegrate the main part of the stone.Residual stones in the inaccessible calyx must preferably be relocated using the "needle technique" to the pelvis and removed via the main access.During PCNLT of coral nephrolithiasis, the frequency of bleeding episodes, the volume of blood loss and the frequency of blood transfusion are significantly lower, the length of hospital stay is shorter than during open interventions.
References
| [1] | Zenkov S. S., Berestennikov K. A., Prityko A. A. Analysis of complications of percutaneous X-Ray endoscopic surgical operations of patients with urolithiasis and nephrolithiasis with a single functioning kidney // Andrology and Genital Surgery. – 2015. – Т. 16. – №. 1. – С. 49-52. |
| [2] | Alyayev YU.G., Glybochko P.V. Urolithiasis disease. Modern view of the problem. Guide for doctors. 2016: 1-148. |
| [3] | Taguchi, K., Yasui, T., Milliner, D.S., Hoppe,B., Chi, T. Genetic Risk Factors for idiopathic Urolithiasis: A systematic review of the literature and causal network analysis. // European Urology Focus. Volume 3, Issue 1, February 2017, Pages 72-81 https://doi.org/10:1016/j.euf.2017.04.010. |
| [4] | Feofilov I. V. Surgery of coral nephrolithiasis //Journal of siberian medical sciences. – 2015. – Т. 4. – С. 18. |
| [5] | Kalinina S. N. et al. Experience of treating patients with urolithiasis in the urological clinic of the Aleksandrovskaya hospital // Urology reports (St.-Petersburg). – 2019. – Т. 9. – №. 3. – С. 21-28. |
| [6] | Alsagheer G. et al. Extracorporeal shock wave lithotripsy (ESWL) monotherapy in children: Predictors of successful outcome // Journal of Pediatric Urology. – 2017. – Т. 13. – №. 5. – С. 515. e1-515. e5. |
| [7] | Atduev V. A. et al. Percutaneous nephrolitholapaxy performed under ultrasound and endovisual guidance: evaluation of the factors affecting the immediate outcomes // Urology Herald. – 2022. – Т. 10. – №. 2. – С. 5-18. |
| [8] | Glybochko P. V. et al. Laparoscopic pyelolithotomy and its role in modern surgery of nephrolithiasis // Urologiia (Moscow, Russia: 1999). – 2017. – №. 4. – С. 12-17. |
| [9] | Glybochko P. V. et al. Laparoscopic pyelolithotomy and its role in modern surgery of nephrolithiasis // Urologiia (Moscow, Russia: 1999). – 2017. – №. 4. – С. 12-17. |
| [10] | Protoshak V. V. et al. Percutaneous Urolithiasis Surgery in Military //Bulletin of the Russian Military Medical Academy. – 2020. – Т. 22. – №. 3. – С. 29-34. |
| [11] | Аkilov F. Complications of extracorporeal shock-wave lithotripsy and their systematization. – 2021. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML