-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(12): 1292-1296
doi:10.5923/j.ajmms.20221212.24
Received: Nov. 24, 2022; Accepted: Dec. 10, 2022; Published: Dec. 23, 2022

Origin, Nature and Consequences of Modern Mechanical Trauma
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIndiaminov Sayit Indiaminovich1, 2, Norkulov Urol Farxadovich3
1Republican Scientific and Practical Center of Forensic Medical Expertise of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
2Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
3Samarkand Branch of the Republican Scientific and Practical Center of Forensic and Medical Expertise, Samarkand, Uzbekistan
Correspondence to: Indiaminov Sayit Indiaminovich, Republican Scientific and Practical Center of Forensic Medical Expertise of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

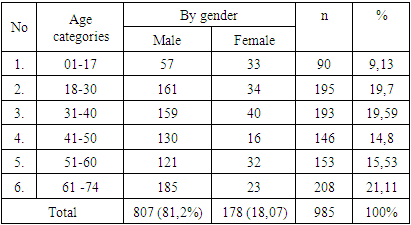
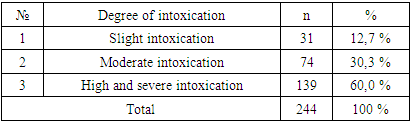
In order to identify the circumstances, structure and consequences of a mechanical injury, a retrospective analysis of the conclusions of the forensic medical examination over the past 5 years (2017-2021) was carried out. It was found that the majority of death cases from mechanical trauma was made up of males (81.2%) at the most working age of 18-60 years (90.73%). Deceased children amounted to 9.13%. The share of people who died over 60 years old fell 21.11% of cases. It was revealed that the largest number of fatal mechanical injuries was due to road accidents (67.4%), of which 65.4% are car injuries. In 62.2% of cases, the victims died at the scene of injury, in the remaining 37.8% of cases, mortality occurred in medical institutions. The largest number of deaths from mechanical trauma were in a state of high and severe intoxication (60.0%). At the same time, in 12.7% of cases of establishment of mild and 30.3% of medium degree intoxication. In the conditions of an accident and during falls, the victims had a combined and multiple trauma, covering more than 2 parts of the body, which were dominated by craniocerebral trauma, then injuries to the chest, abdomen and limbs.
Keywords: Mechanical trauma, Origin, Character, Death, Causes, Diagnosis
Cite this paper: Indiaminov Sayit Indiaminovich, Norkulov Urol Farxadovich, Origin, Nature and Consequences of Modern Mechanical Trauma, American Journal of Medicine and Medical Sciences, Vol. 12 No. 12, 2022, pp. 1292-1296. doi: 10.5923/j.ajmms.20221212.24.
Article Outline
1. Actuality of the Problem
- The modern era is characterized by a steady increase in traumatism associated with a sharp increase in the number of road traffic accidents (accidents) and catatraumas. In the structure of damage by blunt mechanical factors, the leading place is occupied by the number of victims of combined and multiple injuries. Around the world, about 5.8 million people die annually from similar injuries, among whom people of the most working age predominate. Mortality caused by combined trauma in specialized clinics is 18.8-36.0% and 50-60% of victims die at the prehospital stage. In this regard, injuries around the world are the most pressing socio-demographic, medical-biological and economic problem. [4,6,11,13,17,18,21].These data dictate the need for further improvement of methods of prevention, diagnosis, treatment and rehabilitation of patients with combined trauma. In this regard, an important role is played by the analysis of the results of forensic medical examinations (SME) related to the fatal outcomes of mechanical trauma, the results of which can become the basis for the development of preventive measures, as well as the improvement of adequate methods of treating patients with injuries of varying severity.Objective - to identify the circumstances, structure and consequences of mechanical trauma.
2. Materials and Methods of Research
- A retrospective analysis of the data of the conclusions of forensic medical examinations of corpses conducted in the Samarkand branch of the Republican Scientific and Practical Center for Forensic Medical Examination of the SME of the Republic of Uzbekistan for the period 2017-2021 (5 years) was carried out. In the process of analysis, the circumstances of injuries, the dynamics of mortality rates by year, by sex and age of the victims, as well as the nature and volume of lesions of individual parts of the body and the causes of death were revealed. Within the framework of variational statistics, the criterion of reliability of indicators (t) their minimum error (m) and reliability (p) differences in indicators were determined.
3. Research Results and Discussion
- It was established that during this period 2256 studies of the corpses of persons who died from diseases and injuries were carried out. Of these, 985 cases (44%) were associated with the death of victims of exposure to mechanical factors, the distribution of which by sex and age is given in Table No. 1.
|
|

|
4. Conclusions
- 1. In the materials of forensic medical examination, fatal mechanical trauma accounts for 44% of the total number of expert studies conducted. The majority of those died from mechanical trauma are males (81.2%) at the most working age -18-60 years (90.73%).2. The main number of mechanical injuries was caused by road accidents (67.4%), of which 65.4% is a car injury. In 62.2% of cases, victims with mechanical trauma died at the sites of injury, in the remaining 37.8% of cases, mortality was received in medical institutions. During a forensic chemical study in the blood and urine of 24.8% of the dead, ethyl alcohol was found, the concentration of which in the blood of most of the dead corresponded to a strong and severe degree of intoxication. 3. The nature, location, severity and extent of body injuries in the deceased depended on the type of injury. In the conditions of transport trauma, basically, combined or multiple injuries were detected, covering more than 2 parts of the body, which were dominated by craniocerebral traumas (CCT), then - the chest, abdomen and limbs. A similar nature of the injuries occurred during the falls of the victims from a height, but CCT and injuries of the musculoskeletal system prevailed. At the death of victims from the effects of various blunt objects, tools, including parts of the human body during illegal actions, CCT and injuries to internal organs, mainly abdominal organs, prevailed. 4. Injuries to the structure of the head and its facial section (open, closed CCT) were detected in 58% of the victims. At the same time, CCT conditions in 40% of the dead were accompanied by lesions of the bones of the skull and in the remaining 60% of cases - CCT occurred with severe brain contusion and under the sheathing, as well as intracerebral hemorrhages, which were the direct cause of death of the victims at the pre-hospital stage.5. In the earlier period of CT (1-3 days), the death of the victims occurred as a result of edema and dislocation of the brain, ascending edema of the spinal cord, traumatic and hemorrhagic shock, pulmonary edema, fatty embolism of the vessels of the brain and lungs, and in the distant period (over 3-7 days) of trauma - as a result of purulent-septic complications, pulmonary embolism or decompensation of somatic chronic diseases of the heart, lungs, liver and kidneys.6. With damage by sharp objects, hollow-cut penetrating wounds with damage to internal organs prevailed. The immediate causes of death of the victims were massive blood loss, hemo and pneumothorax, cardiac tamponade and, in some cases, air embolism. With a gunshot injury, the death of the victim occurred as a result of through gunshot wounds to the chest and abdomen with damage to internal organs, complicated by massive blood loss, hemo and pneumothorax.7. These data should be taken into account in the process of forensic diagnosis of mechanical trauma, as well as in the provision of emergency and emergency medical care to victims and in the development of preventive measures to prevent injuries. To establish the role of injuries of individual structures in the mechano- and thanatogenesis of traumatic illness, it is necessary to conduct a detailed analysis of the nature of the volume and complication of damage to various parts of the body.