-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(12): 1180-1184
doi:10.5923/j.ajmms.20221212.02
Received: Nov. 10, 2022; Accepted: Nov. 25, 2022; Published: Dec. 9, 2022

Determination of the Origin of the Disease Against the Background of Hyperhomocysteinemia, Changes in Folic Acid and Vitamin B12 Indicators in Patients with Ischemic Stroke
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLVakhabova Nargiza Maksudovna
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Vakhabova Nargiza Maksudovna, Tashkent Medical Academy, Tashkent, Uzbekistan.
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Modern literature sources devoted to one of the most important risk factors for cerebrovascular diseases, hyperhomocysteinemia, are analyzed. The incidence of hyperhomocysteinemia in various subtypes of ischemic stroke was assessed. Genetic and non-genetic markers of homocysteine metabolism are presented. The factors influencing the change in the concentration of homocysteine in the blood plasma were analyzed. The important role of the amino acid in the physiological processes occurring in the body, as well as in the pathological mechanisms of the formation of cerebrovascular insufficiency, is shown. The existence of a relationship between an increase in the level of homocysteine and the amount of damage to the medulla in patients with an atherothrombotic subtype of stroke has been proven, which in turn proves the importance and necessity of both primary and secondary preventive therapy with B vitamins.
Keywords: Ischemic stroke, Homocysteine, Hyperhomocysteinemia, Stroke subtypes, Vitamin therapy, Prevention of cerebrovascular disease, Markers of homocysteine metabolism
Cite this paper: Vakhabova Nargiza Maksudovna, Determination of the Origin of the Disease Against the Background of Hyperhomocysteinemia, Changes in Folic Acid and Vitamin B12 Indicators in Patients with Ischemic Stroke, American Journal of Medicine and Medical Sciences, Vol. 12 No. 12, 2022, pp. 1180-1184. doi: 10.5923/j.ajmms.20221212.02.
1. Introduction
- Stroke is one of the leading causes of death in any population, and its prevention is a key strategy to reduce mortality and morbidity. According to some authors [1,10], an increase in the level of homocysteine by only 20–30% can lead to irreversible consequences, including ischemic stroke. An increase in the level of blood homocysteine by 5 µmol/l from the upper limit of the norm leads to an increase in the risk of atherosclerotic vascular lesions by 60% in men and 80% in women [12]. It is also known that hyperhomocysteinemia accompanies a number of oncological diseases [2,4]. Hyperhomocysteinemia is a potentially modifiable risk factor for cerebral stroke, however, to date, the fight against an increase in the level of homocysteine is carried out mainly in the framework of secondary prevention in order to reduce the risk of developing a recurrent vascular event. [1]Several risk factors for stroke have been identified and are the target of both primary and secondary prevention strategies. In 1969, McCully showed that elevated levels of total homocysteine are the cause of vascular disease in children with congenital anomalies in vitamin B12 metabolism. Since then, many studies have been conducted to understand the impact of hyperhomocysteinemia on cerebrovascular disease. While some studies have shown that homocysteine is an independent risk factor, others have not. [5]Deficiency of almost any vitamin can lead to neurological disorders, however, in practice, metabolic disorders of B vitamins (thiamine, pyridoxine (vitamin B6), cyanocobalamin (vitamin B12)), vitamin E and folic acid are of the greatest importance. These vitamins are involved as coenzymes in a variety of redox reactions. [7] This explains the fact that they are critically important in the energy supply of the tissue of the peripheral and central nervous system. Of particular importance in terms of the occurrence of cognitive impairment is given to a deficiency of vitamin B12, folic acid, as well as an increase in the level of homocysteine.Hyperhomocysteinemia can cause endothelial dysfunction due to oxidative stress, leading to local thrombosis and subsequent ischemia. [9] Another possible mechanism is direct vascular toxicity of homocysteine, but there is no definitive evidence to support any of these mechanisms.Homocysteine levels can be influenced by several factors, among which the concentrations of B vitamins, especially B12 and folic acid, are the most important. A decrease in serum levels of these factors leads to an increase in plasma homocysteine levels.Since 1998, fortification of cereal flour products with folic acid has been mandated in the United States to reduce the risk of neural tube defects in newborns. Folic acid supplementation resulted in a decrease in homocysteine levels and cerebrovascular disease by about 20-25%. But some other trials, such as the Vitamin Intervention for Stroke Prevention (VISP), have not confirmed this. [1-4]Two strong determinants of fasting homocysteine concentrations are age and gender, so concentrations are higher in the elderly and higher in men than women. In addition, there is a strong negative correlation between estradiol levels and homocysteine levels in postmenopausal women. Therefore, hormone therapy can lower homocysteine levels. [8] Some studies have shown that smokers have higher levels of homocysteine than non-smokers, regardless of age or gender. Drinking a lot of coffee is one of the strongest lifestyle determinants of homocysteine levels. In addition, both exercise and alcohol consumption are weak but important determinants of homocysteine. Findings from cross-sectional and population studies have shown that changes in some of these lifestyle factors, such as higher intake of B vitamins, smoking cessation, and coffee abstinence, can lead to lower homocysteine concentrations over time. [11]The aim of this study was to determine if there is a significant difference in levels of homocysteine, folic acid, and vitamin B12 between stroke patients and healthy controls.
2. Materials and Methods
- This study was conducted in the Department of Intensive Care and Neurology of Clinic No. 1 of the Tashkent Medical Academy. The control of this condition was compared with 93 patients hospitalized with ischemic stroke, grade I-II dyscirculatory encephalopathy who were hospitalized in the neurology department between January 2021 and September 2022, by age and gender with 53 patients from the same hospital, in who did not have acute cerebrovascular disease.Informed consent was obtained from all stroke patients or their proxies, as well as from all healthy controls. Data (collected from case and control groups) included age, sex, body weight, history of blood pressure and/or hypertension, diabetes mellitus, smoking, alcohol use, previous thrombotic episodes, and history of oral contraceptive use in women. Patients who had conditions (or were taking certain medications) that affect homocysteine levels, including kidney failure requiring dialysis, the use of methotrexate, tamoxifen, L-DOPA, phenytoin, or bile acid sequestrants, were excluded.The antecubital area of either arm was used as the first choice for venipuncture and (after 12 hours of fasting) blood samples were taken. The blood sample was centrifuged as soon as possible, but it could be stored on wet ice for up to 6 hours. Plasma was aliquoted, frozen for 12 hours, and shipped the next day on dry ice to the central laboratory. the levels of homocysteine, vitamin B12 and folic acid were determined by ELISA. Hyperhomocysteinemia was defined as a plasma homocysteine level above 14 limol/L.The statistics in this study were made using the SPSS software (version 16.0). Comparison of serum levels of the three major factors between cases and controls was performed using a t-test.
3. Results
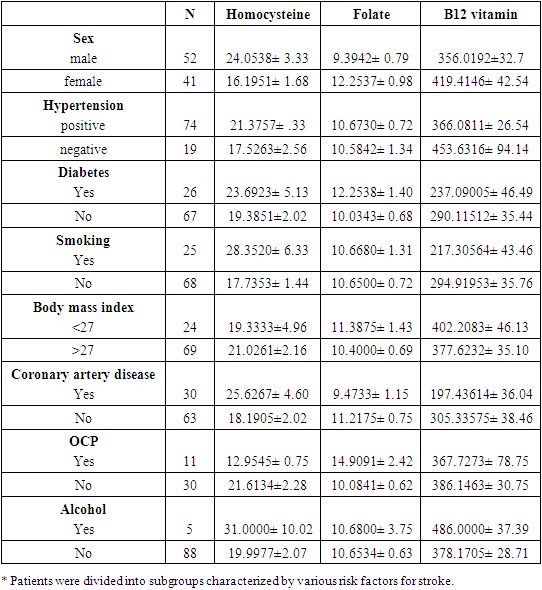
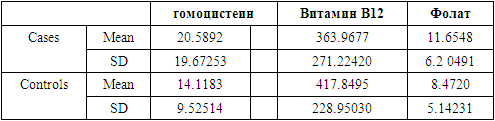
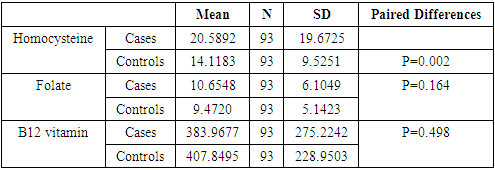
- In total, the study involved 93 patients with acute ischemic stroke (42 women and 51 men) and 53 healthy people (24 women and 29 men). The mean age ± standard deviation of patients and controls was 47.8 ± 6.8 years and 49.8 ± 6.9 years, respectively (T = 0.32, P = 0.75). There was no significant difference between the mean age ± SD of male (47.0 ± 3.5) and female (46.7 ± 9.0) stroke patients (T = 0.69, P = 0.49).The values of homocysteine, folic acid and vitamin B12 in groups of patients characterized by various risk factors for stroke are presented in Table 1. Table 2 shows the mean values and standard deviation of the levels of homocysteine, vitamin B12 and folic acid in blood serum. The average fasting homocysteine level ± standard deviation in patients with acute ischemic stroke was 20.58 ± 19.6 pmol/l, which was significantly higher than its level in the control.
|
|
|
4. Discussion
- In this study, 41% of patients had hyperhomocysteinemia. The main results were as follows: (i) plasma levels of homocysteine in the acute phase of ischemic stroke (within 24 hours) were significantly above normal limits. (ii) No correlation was observed between homocysteine levels and stroke risk factors such as hypertension, hyperlipidemia, diabetes mellitus, alcohol use, coronary heart disease, and obesity. (iii) homocysteine levels were significantly higher in smokers than in non-smokers. (iv) No association was found between serum levels of vitamin B12 and folic acid and risk factors. (v) No significant differences in serum vitamin B12 and folic acid levels were observed between patients and controls.Parnetti et al. studied 121 consecutive patients with first-time ischemic stroke classified using the TOAST criteria and 112 neurologically healthy controls to assess the association between stroke risk and elevated plasma homocysteine and the interaction between mild hyperhomocysteinemia and normal vascular events. risk factors. homocysteine was elevated in all stroke subtypes: 13.0±2.5 gmol/l in patients with cardioembolism, 13.9±5.4 gmol/l in small vessel diseases, 15.5±6.8 gmol/l in undetermined stroke and 17.8±13.5 gmol/l. /l in patients with lesions of large vessels. The average level of homocysteine was 8.10 gmol/l (SD=2.5) in the control. They suggested that mild hyperhomocysteinemia plays a significant role as a risk factor for all etiological subtypes of stroke.Although we did not sort our cases by their subtypes, we arrived at the same result as Parnetti et al. We both found that homocysteine levels are significantly higher in stroke patients than in controls, and this may be a risk factor for stroke.In a prospective study by Perini et al. measured plasma homocysteine levels in stroke patients to investigate possible correlations of homocysteine with stroke severity and clinical outcome. Plasma Hcy was not an independent determinant of stroke severity and disease outcome as measured by the Barthel index. The mean plasma homocysteine level in both ischemic and hemorrhagic stroke was significantly higher than in controls (P<0.05). Homocysteine in the acute phase of stroke was not associated with stroke severity or outcome. Elevated plasma homocysteine levels during the acute phase of stroke have been associated with both ischemic and hemorrhagic stroke. Higher levels were associated with a higher risk of the small artery stroke subtype. They failed to demonstrate that patients with high homocysteine levels in the acute phase of ischemic stroke have a worse outcome. According to their study, hyperhomocysteinemia has no prognostic value. [7]We assessed plasma homocysteine levels in the acute phase of ischemic stroke but did not assess stroke severity or outcome in this study. Despite this, the main conclusion of Perini et al. was the same as in our study; that is, an elevated plasma homocysteine level in the acute phase of a stroke.In 2005, Haapaniemi et al. [8] measured plasma homocysteine levels in 102 consecutive stroke patients on admission, 1 week, 1 month, and 3 months after stroke, and only once in 102 controls. Compared with the control group, plasma homocysteine levels in patients were significantly lower at admission, but not at later times, with levels increasing every week and remaining at this level for 3 months. Homocysteine levels showed a positive correlation with age and a negative correlation with Mini Mental State Test (MMSE) scores. Plasma homocysteine levels were inversely correlated with plasminogen activator inhibitor. There was no correlation between homocysteine levels and stroke severity, outcome, etiology, recurrence, infarct volume, CRP, or risk factors. They suggested that this phenomenon was due to an acute phase response reflecting increased synthesis of acute phase proteins. However, they were unable to find any correlation between acute stroke CRP concentrations and homocysteine levels, which confirms earlier results. [1]This study assessed the relationship between stroke risk factors and the mentioned serum factors. Like Haapaniemi et al., [8] our study showed no correlation between homocysteine levels and most cerebrovascular risk factors. But there was one difference: we found that homocysteine levels were significantly higher in smokers than in non-smokers.
5. Conclusions
- Overall, it can be concluded that elevated plasma homocysteine may be an independent risk factor for ischemic stroke. But, since this study was a case-control study, we could not rule out the possibility that the acute phase reaction is responsible for the increase in serum homocysteine levels in patients with acute stroke. More prospective and population-based studies are needed to determine whether elevated plasma homocysteine is an independent risk factor for cerebrovascular disease or whether stroke itself is a cause of hyperhomocysteinemia.