Shoira U. Babadzhanova1, Tulkin K. Nosirov2, Navrozbek Z. Kahharov3
1Department of Medical Law, Pathological Anatomy, Forensic Medicine, Termez Branch Tashkent Medical Academy, Uzbekistan
2Department of Forensic Medicine and Medical Law, Tashkent Pediatric Medical Institute, Uzbekistan
3Department of Pathological Anatomy, Forensic Medicine, Medical Law, Termez Branch Tashkent Medical Academy, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The material for the study was forensic medical examination of the corpses of people who died from acute and chronic drug poisoning, which were divided into the following groups: 1) acute drug poisoning - 18 cases (25%) ended in death; 2) 53 cases (75%) of non-fatal intoxications. The collected materials were analyzed: case histories, conclusions of forensic chemical analyzes of blood and urine of victims of acute drug poisoning, in order to establish the risk of mortality depending on the concentration of morphine in the blood. In all cases, opiate poisoning was verified by the case materials, the clinical picture of intoxication, and intravital quantitative detection of opiates and their metabolites in the blood and urine.To obtain the necessary information, according to the forensic chemical analysis, the initial level of the main metabolite of opiates, morphine, in the blood (in units of SI-µg/ml) was established. Thus, we have constructed probit-graphs poison concentration-effect. Based on the obtained graphical data, the possibility of death in a different range of poison concentrations was assessed. On the abscissa axis of the graph, a coordinate point corresponding to the level of morphine in the blood was determined, and a perpendicular was mentally drawn until it intersects with the curve of the graph, then continuing it with a parallel (horizontal) line to the left until it intersects with the y-axis. The points of intersection of this conditional line with the y-axis corresponded to the risk of death at this concentration of morphine in the blood. Thus, it is possible to determine the immediate cause of death, based on the concentration of morphine.The developed probit-graphs of the “poison concentration-effect” dependence allow for a quantitative assessment of the risk of death in the entire range of morphine concentrations in the blood, and this makes it possible to determine the severity of a chemical disease (threshold, critical, fatal). Comparison of the main morphological manifestations of opiate poisoning with the immediate causes of death of the victims and the clinical picture of poisoning makes it possible to determine the main types of thanatogenesis, and each type of death has its own characteristic complex of clinical and morphological features. This enables the forensic expert to objectively establish not only the main cause of death, but also the type of thanatogenesis indicating the direct cause of death.
Keywords:
Probit-plot, Concentration thresholds, Structural portrait of a chemical disease, Characteristic and cluster analyses, Thanatogenesis
Cite this paper: Shoira U. Babadzhanova, Tulkin K. Nosirov, Navrozbek Z. Kahharov, Forensic Aspects of Toxicometric Assessment of Acute Poisoning with Narcotic Substances, American Journal of Medicine and Medical Sciences, Vol. 12 No. 10, 2022, pp. 1090-1098. doi: 10.5923/j.ajmms.20221210.18.
1. Introduction
The history of the emergence, distribution, medical use, and then the non-medical "development" of opiates has at least 5,000 years. One of the widely used drugs are opiates - opium surrogates, morphine and heroin. Drug addiction is one of the main medical and social problems of our time. Its spread leads to a continuous increase in mortality from acute drug poisoning, as well as from complications of chronic drug intoxication [1,3,12]. Currently, the number of cases of drug poisoning is continuously growing [4,5,6,8,9]. They occupy a significant place both in the total number of all poisonings and in the entire forensic structure of mortality in general. Articles published on this subject indicate a sharp increase in cases of overdoses of narcotic drugs. The number of cases of detection of toxic concentrations of narcotic substances in the blood and urine of victims with other causes of death is also growing. At the same time, the greatest number of deaths as a result of acute poisoning with these poisons falls on the age from 17 to 23 years and reaches 42% of the total number of fatal poisonings [2,7,11].Acute poisoning, like other types of violent death, is the subject of forensic research. Currently, forensic medical diagnosis of fatal poisoning by narcotic and psychotropic substances is exclusively based on the results of a forensic chemical analysis of blood and urine. At the same time, all cases of a positive determination of opiate metabolites in the blood, urine and internal organs often come down to the verdict of a forensic physician that death was caused by drug poisoning.However, it should be borne in mind that the detection of a toxic substance in a biomaterial does not always indicate poisoning. In this regard, the search for new quantitative expert criteria for assessing acute drug poisoning is a very urgent problem in forensic medicine.The purpose of the study is a toxicometric analysis of clinical and morphological parameters in acute drug poisoning and the development of quantitative criteria for diagnosing and assessing the severity of a chemical disease.
2. Materials and Research Methods
The material for the study was forensic medical examination of the corpses of people who died from acute and chronic drug poisoning, which were divided into the following groups: 1) acute drug poisoning - 18 cases (25%) ended in death; 2) 53 cases (75%) of non-fatal intoxications. (See Fig. No. 1). | Figure 1. Distribution of victims by poisoning groups (1.2) |
The collected materials were analyzed: case histories, conclusions of forensic chemical analyzes of blood and urine of victims of acute drug poisoning, in order to establish the risk of mortality depending on the concentration of morphine in the blood. In all cases, opiate poisoning was verified by the case materials, the clinical picture of intoxication, and intravital quantitative detection of opiates and their metabolites in the blood and urine.
3. Research Results
The key point in the diagnosis of fatal poisoning is the result of a forensic chemical determination of the metabolic products of a chemical in tissues and organs. At the same time, it is not clear why all cases of positive determination of opiate metabolites in the blood, urine and internal organs should be attributed to a single category - those who died from acute opiate poisoning. The qualification of opiate poisoning almost always depends on how we evaluate the level of morphine in the urine, blood and sometimes in the internal organs, then in practice the solution to the question of exactly fatal poisoning comes down to clarifying the question - could the detected concentration of morphine cause death, and if so, then what morphological manifestations should this condition be accompanied by. To obtain the necessary information, according to the forensic chemical analysis, the initial level of the main metabolite of opiates, morphine, in the blood (in units of SI-µg/ml) was established. Thus, we have built probit-graphs "poison concentration-effect".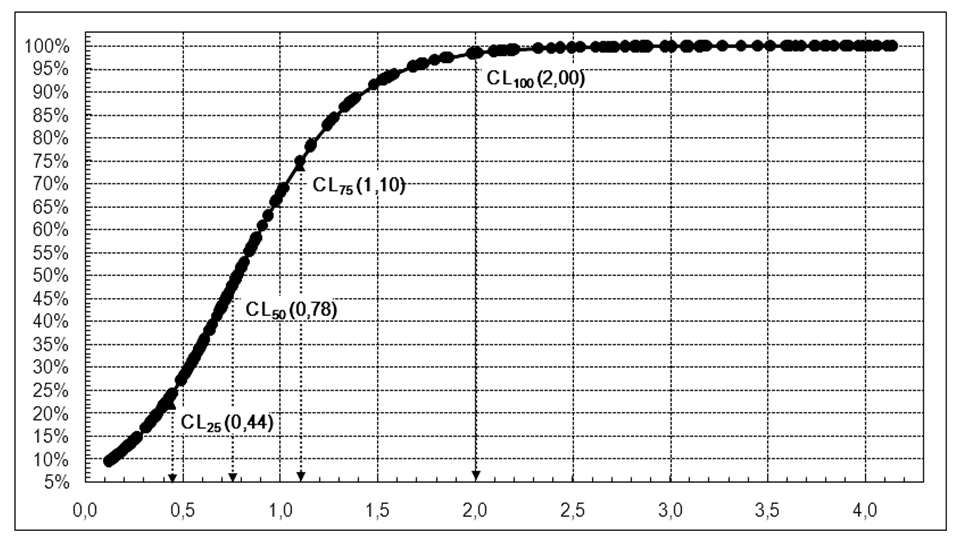 | Figure 2. Probit-graph of dependence of the risk of lethality (%) on the concentration of total morphine in blood plasma (mcg/ml) "poison concentration-effect" |
According to the obtained graphical data, the possibility of death in a different range of poison concentrations was assessed. On the abscissa axis of the graph, a coordinate point corresponding to the level of morphine in the blood was determined, and a perpendicular was mentally drawn until it intersects with the curve of the graph, then continuing it with a parallel (horizontal) line to the left until it intersects with the y-axis. The points of intersection of this conditional line with the y-axis corresponded to the risk of death at this concentration of morphine in the blood. Thus, it is possible to determine the immediate cause of death, based on the concentration of morphine. The immediate cause of death in the first 72 hours was acute intoxication leading to respiratory paralysis (34.6%). In more distant periods, death was associated with pneumonia (22.3%), myocardial dystrophy (5.6%), sepsis (5.6%).In all cases, during a forensic chemical study, morphine was detected in the blood (n=48) (1.5±0.06 µg/ml), in 13 victims (27%), morphine was also detected in the urine (from 1.8 ± 0.04 μg/ml to 4.6 ± 0.8 μg/ml).In addition, using this method, we conducted additional analyzes of the risk of death for men and for women, as well as depending on age. (Fig. No. 3,4)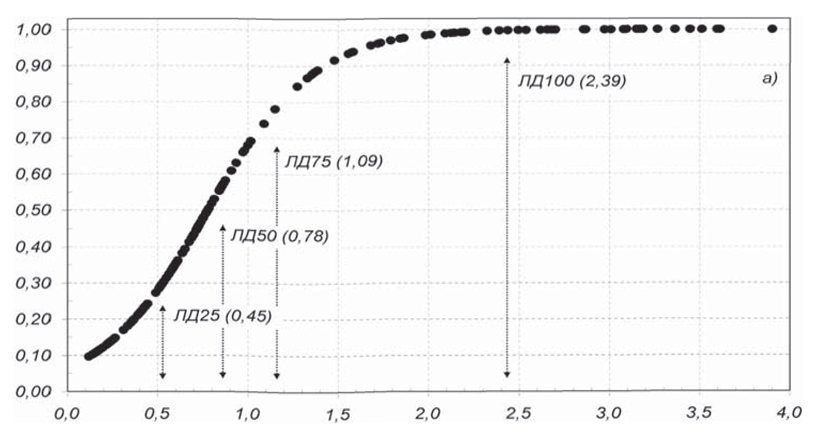 | Figure 3. Probit plot of risk of death versus total morphine blood concentration (µg/mL) in men |
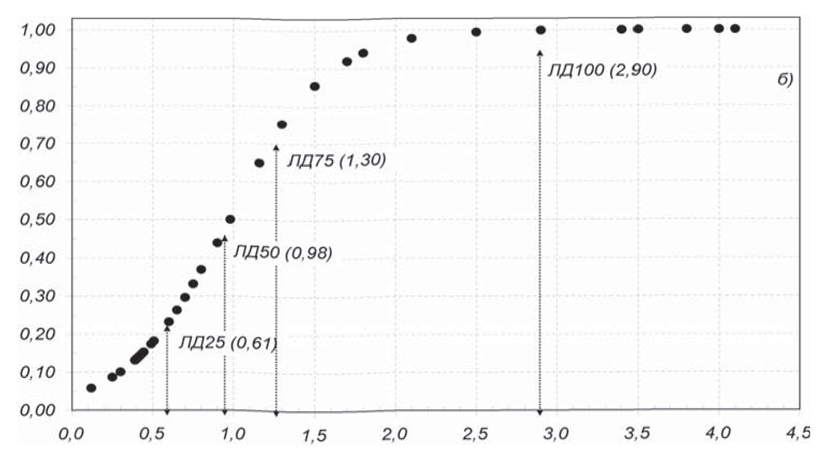 | Figure 4. Probit plot of total blood morphine (µg/mL) risk of death versus poison concentration-effect concentration in women |
The spread of concentrations in both men and women was almost the same, however, as the probit graphs show, the prognosis of the risk of death in men is much higher. In these graphs, it is more shifted to the left. In addition, they show that the critical concentration of morphine in the blood of women (Cn50) was 0.98 µg/ml, while in the blood of men the lethal concentration was much lower and amounted to 0.78 µg/ml. The results of a comparative analysis of probit-graphs of the dependence of the risk of death on the concentration of total morphine in the blood showed that the woman's body has a greater resistance to the action of opiates in the zone of high concentrations, however, as the level of poison in the blood increases, the sex differences in the possibility of survival smooth out.Next, we carried out a comparative analysis of the probit-graphs of the “poison concentration-effect” dependence in the age aspect (Fig. 5, 6). All victims were divided into 2 groups: 1) under 25 years old; 2) over 25 years old. Studies have shown that the risk of death from acute opiate poisoning in people under 25 years of age is significantly higher than in victims over 25 years of age. Thus, the average content of morphine in the blood of victims under the age of 25 in our observations was 0.58 ± 0.04 μg/ml, and in the blood of victims over the age of 25 years it was 1.17 ± 0.06 μg/ml.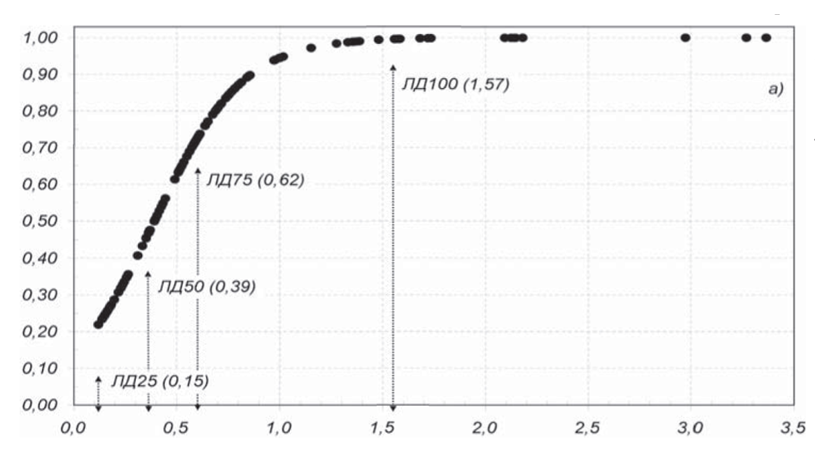 | Figure 5. Probit plot of the "poison concentration-effect" dependence in victims under the age of 25 years |
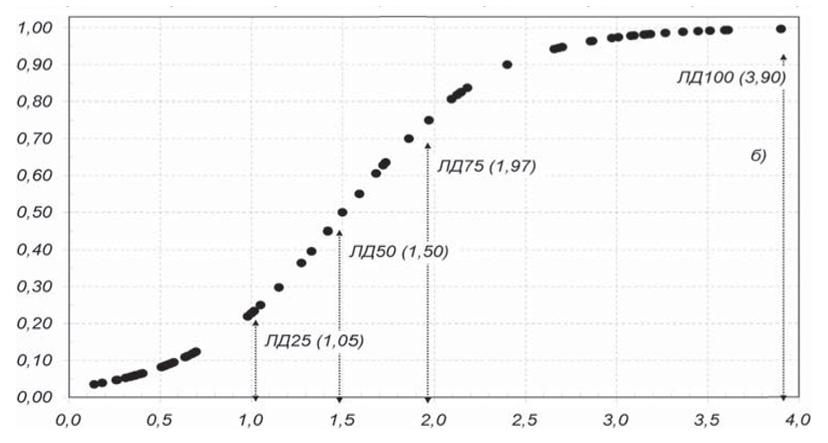 | Figure 6. Probit plot of the "poison concentration-effect" dependence in victims over the age of 25 years |
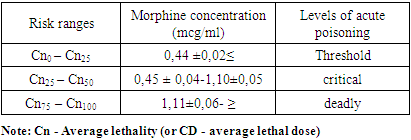
The given probit graphs show that the toxicity of opiates in these age groups with the same parenteral intake of opiates into the body is unequal. The higher the age, the higher the level of morphine in the blood, which is 0.5 μg / ml, much lower than even the dose of C25, at which the risk of death is not so great, and for people under 25 years old, this level approaches C75, corresponding to the critical level. In addition, in the age group up to 25 years, the probit curve is noticeably shifted to the left, which indicates a much higher risk of death for this group in a narrow range of morphine concentrations in the blood (Cn50 = 0.62; Cn70 = 1.57 μg / ml), while in the age group over 25 years, the outcome of the course of poisoning is in most cases uncertain, and the critical level is 3.9 ± 1.04 μg / ml, corresponding to a dose of Cn75-100.Therefore, in our opinion, it is unacceptable to unambiguously interpret the results of a positive forensic chemical analysis as evidence of fatal opiate poisoning, especially if their metabolites are determined only in the urine. The developed probit-graphs of the “poison concentration-effect” dependence allow for a quantitative assessment of the risk of death in the entire range of morphine concentrations in the blood, and this makes it possible to determine the severity of a chemical disease (threshold, critical, fatal). When establishing a diagnosis of opiate poisoning, the expert should focus on these parameters (Table No. 1).Table 1. Morphine risk ranges by parameters of blood morphine concentrations
 |
| |
|
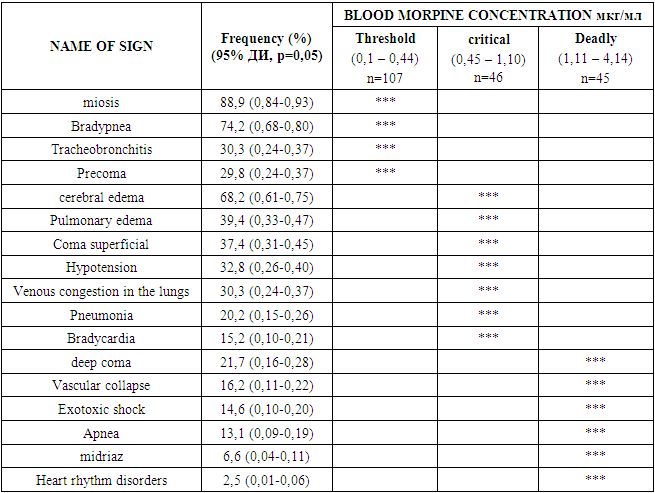
The results of the post-mortem detection of opiate drugs (morphine) in the urine (or in other biological media) can only be used as a fact of drug intoxication, confirming the use of opiates before death.In order to determine the possible ways of the mechanism of thanatogenesis of death in cases of opiate poisoning, the clinical picture of poisoning and the level of decompensation of the main body systems, including the central nervous system, respiratory and cardiovascular systems, were studied. The data obtained were compared with the concentration of total morphine in blood plasma, i.e. determined the concentration thresholds of clinical signs in these acute intoxications.The results of the study showed that in the clinical course of acute opiate poisoning, rather specific lesions are detected: depression of the central nervous system and respiration, hemodynamic disturbances, miosis, and cardiac arrhythmias. All these clinical symptoms in their totality are the toxic effect of acute intoxication.The greatest changes among the symptoms of CNS lesions were associated with impaired consciousness. The leading role belonged to the exclusion of consciousness by the stem type, stunning, stupor, coma were distinguished, with severe respiratory disorders and deep hypoxia of the brain, a convulsive syndrome arose. Subsequently, at the somatogenic stage of acute poisoning, neurological symptoms were predetermined by cerebral edema and impaired cerebral circulation (Table No. 2).Table 2. Concentration thresholds for clinical signs of acute opiate poisoning
 |
| |
|
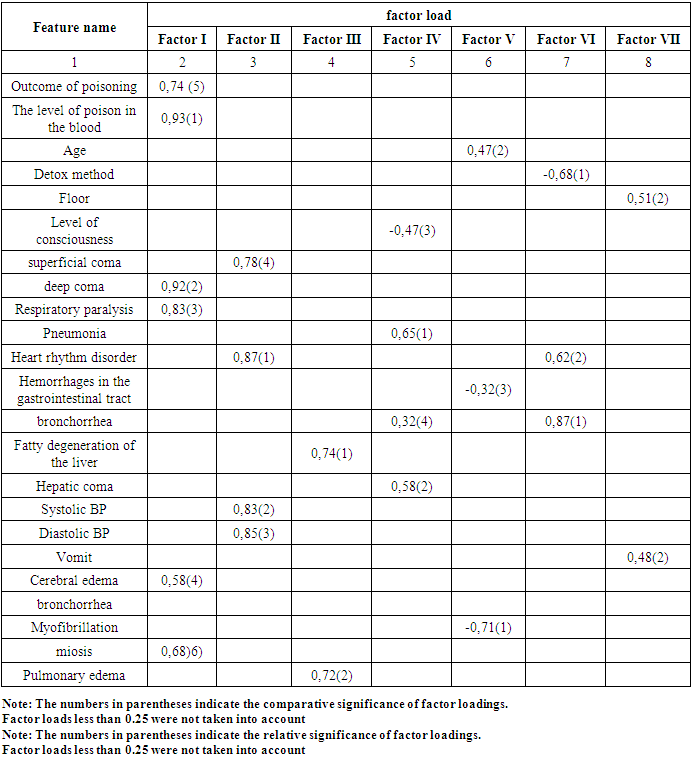
Analysis of the data presented in Table No. 2 shows that at threshold concentrations of the poison in the blood plasma, clinical symptoms are minimal and manifest mainly by specific signs, however, as the concentration of morphine increases, the syndrome complex of the body's response becomes nonspecific.For an objective assessment of the body's response to chemical injury, methodologically, the method of factor analysis is most suitable, the essence of which in the medical presentation is the construction of mathematical structures - interconnected (correlating) signs, combined, according to the principle of commonality of changes in the pathological process into factors. Using this method, one can not only establish causal relationships, but also quantify them. Thanks to this, the analysis becomes objective and accurate, and the conclusions are justified and reliable (see Table No. 3).Table 3. Factor structure of the clinical and morphological picture of acute opiate poisoning
 |
| |
|
The most significant features of opiate poisoning contain factor I. The composition of the elements of this factor reflects both the etiology and the main dependence on the outcome - the concentration of the poison in the blood. The structure of common II, III factors confirms that the body's response is of an integral nature, where the leading element is the inhibition of the activity of the central nervous system (this is evidenced by the value of the factor load of deep coma - 0.92). On the contrary, generalized factors IV, V and other manifestations of opiate poisoning (cardiac arrhythmias, respiratory disturbances, hemorrhages in the gastrointestinal tract, etc.) are not informative signs, since they do not have an independent effect on the outcome of poisoning.Our multidimensional factorial analysis of the clinical course of acute opiate poisoning revealed both specific and nonspecific signs. However, to combine all these features according to the principle of similarity, it is necessary to classify them using cluster analysis (see Fig. No. 7).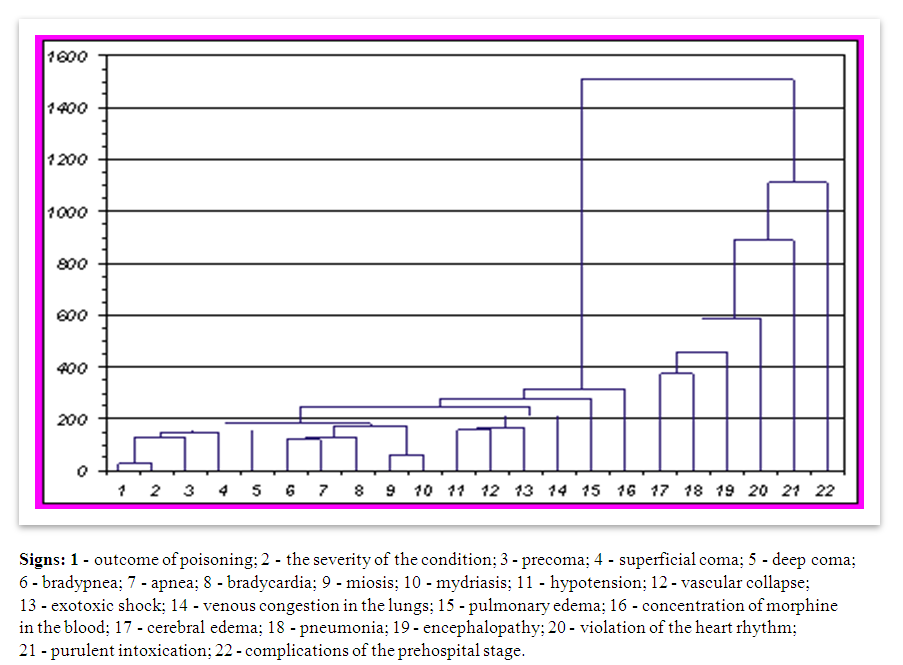 | Figure 7. Dendrogram of functional relationships in acute opiate poisoning |
This dendrogram shows not only the complexity, but also a certain hierarchical ordering of the functional and structural relationships of the body during opiate poisoning. So, for example, in one zone there are indicators of the function of the central nervous system (oppression of consciousness of different depths). At first they act as independent elements, and later they are combined into graphs corresponding to a certain function of the body, and at the level of intercluster distance they merge together, reflecting their commonality in the neurotoxic effect of opiates.When combining features in a cluster, it always starts with the feature that is presented first as the “outcome of poisoning”, and the sequence of subordinate features located after it is automatically ranked according to their level of proximity to the first one.This dendrogram shows not only the complexity, but also a certain hierarchical ordering of the functional and structural relationships of the body during opiate poisoning. So, for example, in one zone there are indicators of the function of the central nervous system (oppression of consciousness of different depths). At first they act as independent elements, and later they are combined into graphs corresponding to a certain function of the body, and at the level of intercluster distance they merge together, reflecting their commonality in the neurotoxic effect of opiates.As this dendrogram shows, in acute opiate poisoning, two local groupings of signs are distinguished - 1-16 and 17-22. To the first group when combining features in a cluster, it always starts with the feature that is presented first as the “outcome of poisoning”, and the sequence of subordinate features located after it is automatically ranked according to their level of proximity to the first one. signs (1-16), in turn, includes three more subgroups - 1-5, 6-10 and 11-14, as well as two separate signs - 15 and 16. There is a very large distance between the left (1-16) and right (17-22) clusters, equal to approximately 1200 units, which indicates that the relationship between these two groups of features is minimal. This dendrogram shows not only the complexity, but also a certain hierarchical ordering of the functional and structural relationships of the body during opiate poisoning. So, for example, in one zone there are indicators of the function of the central nervous system (depression of consciousness of different depths). At first they act as independent elements, but later they are combined into graphs corresponding to belonging to a certain function of the body, and at the level of intercluster distance 160 they merge together, reflecting their commonality in the neurotoxic effect of opiates.The morphological picture of opiate poisoning in fatal cases was characterized by great diversity. However, when comparing the dependence of manifestations of morphological signs with the chronology of poisoning, a certain sequence and interconnectedness of clinical and functional manifestations and their morphological equivalents differed.
4. Discussion
One of the widely used drugs are opiates - opium surrogates, morphine and heroin. Drug addiction is one of the main medical and social problems of our time. Its spread leads to a continuous increase in mortality from acute drug poisoning, as well as from complications of chronic drug intoxication [1,3,12]. Currently, the number of cases of drug poisoning is continuously growing [4,5,6,8,9]. They occupy a significant place both in the total number of all poisonings and in the entire forensic structure of mortality in general. Articles published on this subject indicate a sharp increase in cases of overdoses of narcotic drugs. The number of cases of detection of toxic concentrations of narcotic substances in the blood and urine of victims with other causes of death is also growing. At the same time, the greatest number of deaths as a result of acute poisoning with these poisons falls on the age from 17 to 23 years and reaches 42% of the total number of fatal poisonings [2,7,11].Acute poisoning, like other types of violent death, is the subject of forensic research. Currently, forensic medical diagnosis of fatal poisoning by narcotic and psychotropic substances is exclusively based on the results of a forensic chemical analysis of blood and urine. At the same time, all cases of a positive determination of opiate metabolites in the blood, urine and internal organs often come down to the verdict of a forensic physician that death was caused by drug poisoning.However, it should be borne in mind that the detection of a toxic substance in a biomaterial does not always indicate poisoning. In this regard, the search for new quantitative expert criteria for assessing acute drug poisoning is a very urgent problem in forensic medicine.
5. Conclusions
1. The results of clinical and morphological analysis show that in each specific case, the development of the premortal period is associated with pathological processes that cannot be interpreted unambiguously due to the complexity of developing causal relationships. The main disease, which is acute opiate poisoning, leads to the development of different types of thanatogenesis - cardiac, pulmonary, head, which in turn is characterized by various immediate causes of death.2. According to the obtained graphical data (probit-graphs "poison concentration-effect"), it is possible to assess the possibility of death in a different range of poison concentrations. On the abscissa axis of the graph, a coordinate point corresponding to the level of morphine in the blood was determined, and a perpendicular was mentally drawn until it intersects with the curve of the graph, then continuing it with a parallel (horizontal) line to the left until it intersects with the y-axis. The points of intersection of this conditional line with the y-axis corresponded to the risk of death at this concentration of morphine in the blood. Thus, it is possible to determine the immediate cause of death, based on the concentration of morphine.3. Comparison of the main morphological manifestations of opiate poisoning with the immediate causes of death of the victims and the clinical picture of poisoning makes it possible to determine the main types of thanatogenesis, and each type of death has its own characteristic complex of clinical and morphological signs. This enables the forensic expert to objectively establish not only the main cause of death, but also the type of thanatogenesis indicating the direct cause of death. All this, of course, will increase the objectivity and evidentiary value of forensic medical examinations.4. Analyzes of risk assessment of death in opiate poisoning, the spread of concentrations in both men and women was almost the same, however, as the probit graphs show, the prognosis of the risk of death in men is much higher. In addition, they show that the critical concentration of morphine in the blood of women (Cn50) was 0.98 µg/ml, while in the blood of men the lethal concentration was much lower and amounted to 0.78 µg/ml. The results of a comparative analysis of probit-graphs of the dependence of the risk of death on the concentration of total morphine in the blood showed that the woman's body has a greater resistance to the action of opiates in the zone of high concentrations, however, as the level of poison in the blood increases, the sex differences in the possibility of survival smooth out.5. The developed probit-graphs of the dependence "poison concentration-effect" allow for a quantitative assessment of the risk of death in the entire range of morphine concentrations in the blood, and this allows you to determine the severity of a chemical disease (threshold, critical, fatal). When establishing a diagnosis of opiate poisoning, the expert should be guided by these parameters.The authors declare no conflict of interest.
References
| [1] | Berezovskaya M.A., Karobitsina T.V., Sherstyanykh A.S. Indirect methods for estimating the prevalence of non-medical drug use // Bulletin of the Siberian Legal Federal Drug Control Service of Russia. 2017-№4, pp.106-110. Berezovskaya M.A., Karobitsina T.V., Sherstyanykh A.S. Indirect methods for estimating the prevalence of non-medical drug use // Bulletin of the Siberian Legal Federal Drug Control Service of Russia. 2017 -№4, pp.106-110. |
| [2] | Bonitenko E.Yu. Modeling of toxic coma caused by substances of depritory action // Proceedings of the Institute of Toxicology, dedicated to the 75th anniversary of its foundation / ed. S. Neginorenko. SPb. 2010. С16-30. Bonitenko E. Yu. Modeling of toxic coma caused by substances of depritory action // Proceedings of the Institute of Toxicology, dedicated to the 75th anniversary of its foundation / ed. S. Neginorenko. SPb. 2010. С16-30. |
| [3] | Borodin S.A. Pathomorphology and forensic medical evaluation in acute and chronic combined intoxication with opiates and ethanol: Abstract of the thesis: Candidate of Medical Sciences - Novosibirsk. 2006-S. 21. Borodin S.A. Pathomorphology and forensic medical evaluation in acute and chronic combined intoxication with opiates and ethanol: Abstract of the thesis: Candidate of Medical Sciences - Novosibirsk. 2006-S. 21. |
| [4] | Vaisov S.B. Drug and alcohol addiction: A practical guide-St. Petersburg: Science and technology. 2008 p.268. Vaisov S.B. Drug and alcohol addiction: A practical guide-St. Petersburg: Science and Technology. 2008 p.268. |
| [5] | Veselovskaya N.V., Kovalenko A.E. Drugs. - M.: Triada-X, 2000. - 204 p. Veselovskaya N.V., Kovalenko A.E. drugs. - M.: Triada-X, 2000. - 204 p. |
| [6] | Golovko A.I. Narcology. General issues and pathogenesis of chemical dependence. St. Petersburg: Artik., 2008 P.487. Golovko A.I. Narcology. General issues and pathogenesis of chemical dependence. St. Petersburg: Artik., 2008 P.487. |
| [7] | Kandyba T.S., Dvalidze S.V., Shakhvorostov A.V. Aspects of forensic medical diagnosis of heroin poisoning // Actual issues of theory and practice of Forensic medical examination. Krasnoyarsk. 2007. -Vol.5. Kandyba T.S., Dvalidze S.V., Shakhvorostov A.V. Aspects of forensic medical diagnosis of heroin poisoning // Actual issues of theory and practice of Forensic medical examination. Krasnoyarsk. 2007. -Vol. 5. |
| [8] | Litvitsky P.F. Drug addiction, substance abuse, poisoning // Questions of modern pediatrics. 2004, T.V. No. 3. pp. 51-60. Litvitsky P.F. Drug addiction, substance abuse, poisoning // Questions of modern pediatrics. 2004, T.V. no. 3.pp. 51-60. |
| [9] | Pigolkin Yu. I. Morphological diagnosis of narcotic intoxication in forensic medicine - M.: Medicine. 2004. P.304. Pigolkin Yu. I. Morphological diagnosis of narcotic intoxication in forensic medicine - M.: Medicine. 2004. P.304. |
| [10] | Sivolap Yu.P., Savchenko V.A., Mishnevsky A.L. Multiple lesions of internal organs in opium addiction. // Journal of Neurology and Psychiatry. - 2000. - No. 6. - S. 64-65. Sivolap Yu.P., Savchenko V.A., Mishnevsky A.L. Multiple lesions of internal organs in opium addiction. // Journal of Neurology and Psychiatry. - 2000. - No. 6. - S. 64-65. |
| [11] | Dargam P., Wood D. Novelrecreational drags and "Legal Highs" over the last five years // J. Mod / Toxical. 2010. Number 3. P-236/39. |
| [12] | Harun A. Agbawal Y. The Use of Fall Risk Increasing Drugs (FRIDs) in Patients with Daffiness Presenting to a Neuropathology Clinic. Otolneurotol. 2015. Mat. 30. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML