-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(10): 1086-1089
doi:10.5923/j.ajmms.20221210.17
Received: Oct. 3, 2022; Accepted: Oct. 19, 2022; Published: Oct. 31, 2022

Histotopography of a Nodular Defect of the Interventricular Wall Muscle of the Heart
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRadjabboy I. Israilov1, Javlonbek I. Muydinov2
1Director of the Republican Pathoanatomical Center of the Ministry of Health of the Republic of Uzbekistan
2Independent Researcher, Fergana Medical Institute of Public Health
Correspondence to: Radjabboy I. Israilov, Director of the Republican Pathoanatomical Center of the Ministry of Health of the Republic of Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In this work, the pathomorphological changes in the myocardial tissue surrounding the congenital defect of the interventricular wall muscle part were studied. As a material, fragments taken from interstitial tissue of heart ventricles of children who died from this disease were studied histologically. The results of the research showed that thin rough fibrous connective tissue and endothelium appeared on the surface of the tissue of the edges of the congenital defect of the interventricular wall of the heart ventricles, from which fibrotic tissue bundles spread to the interstitial tissue of the surrounding muscle fibers, and transverse muscle fibers are located in different directions. During the development of the congenital defect, a number of histological defects and deformations are preserved in the myocardial muscle tissue due to the violation of histogenesis and incomplete formation and differentiation of muscle cells even in the preserved muscle tissue of this wall.
Keywords: Heart, Congenital defect, Interventricular wall, Membranous part, Histotopography
Cite this paper: Radjabboy I. Israilov, Javlonbek I. Muydinov, Histotopography of a Nodular Defect of the Interventricular Wall Muscle of the Heart, American Journal of Medicine and Medical Sciences, Vol. 12 No. 10, 2022, pp. 1086-1089. doi: 10.5923/j.ajmms.20221210.17.
Article Outline
1. The Urgency of the Problem
- The muscular, i.e. trabecular, form of congenital defect of the interventricular wall occurs in 15–20%. Such defects are completely surrounded by muscle tissue on all sides and can be located in different areas of the muscle part of the wall, they can be several and can be defined as holes of different sizes. If there are many defects in the muscular part of the wall, it is called Tolochinova–Roje disease. Congenital defects of the wall of the heart ventricles in a child are caused by the use of various drugs and viral infections during pregnancy.The wall separating the left and right ventricles of the heart is actually thick muscle and fibrous tissue. This wall is located in a posterior and rightward direction and bulges toward the right ventricle, and its edges meet the border between the anterior and posterior ventricles [1,2]. The lower part of this wall consists of relatively thick muscle tissue, and the upper part consists of a thin fibrous membrane. The upper part separates the aortic arch from the lower part of the right lobe and is called the membranous septum because it consists of a thin fibrous tissue. The membranous part of the interventricular wall is connected to the fibrous ring of the aortic valve and consists of dense collagen fibers. The wall of the interventricular space is covered with endocardium from both sides, that is, from the left and right ventricles. Endocardial thickness on the left ventricular side, in particular, the interventricular space has a thicker structure in the wall, relatively thin in the entrance hole to the aorta and pulmonary artery and is similar in structure to the structure of the artery wall [3,4]. The surface of the endocardium is covered with an endothelium consisting of polygonal cells, under which there is a thick basement membrane. Underneath the endothelial cells and the basement membrane, a connective tissue consisting of poorly differentiated cells is formed. Under it there is a muscle–elastic layer, where elastic fibers connect with smooth muscle cells and form a mesh. The elastic fibers of this layer are better developed in the compartments compared to the ventricles. The smooth muscle cells of this layer are well developed and have a multi–branched structure at the outlet of the aorta. The deepest part of the endocardium, that is, the part connected to the myocardium, is elastic, consists of connective tissue rich in collagen and reticular fibers. The endocardial tissue is directly nourished by the blood in the ventricles, only the outer connective tissue layer of the endocardium contains blood vessels.The myocardium of the interventricular wall of the heart, like all muscle tissues in the human body, is a tissue with a contractile function using the actin–myosin system in its special myofibrils [5,7,8,9]. The muscle tissue of the heart belongs to the celemic type of transversely propagating muscle tissue and is found only in the myocardial tissue. The peculiarity of this muscle tissue is that actin and myosin myofilaments are located in an important orderly relationship, forming transverse extension lines and providing the property of spontaneous, rhythmic contraction. Such involuntary rhythmic contractions are controlled by the sympathetic and parasympathetic nervous systems.
2. The Purpose of the Study
- Determination of pathomorphological changes in the myocardium tissue surrounding the congenital defect of the interventricular wall of the heart.
3. Material and Methods
- To achieve this goal, we distinguished hearts with congenital holes located in the muscular part of the wall from congenital defects of the interventricular space of the heart. In our hands, there were 12 hearts with a similar congenital defect. First, the diameter and circumference of birth defects-holes were measured using a ruler with millimeter lines and the area of the hole was calculated. Then, the congenital defect–hole was divided into 4 parts together with the surrounding tissue structures and frozen in 10% formalin solution in the form of 4 pieces. Section 1 formed the upper part of the birth defect, section 2 formed the lower part of the birth defect, and sections 3 and 4 formed the sides of the birth defect. Separate histological preparations were prepared from each slice and studied by staining with hematoxylin–eosin.
4. Research Results and Their Discussion
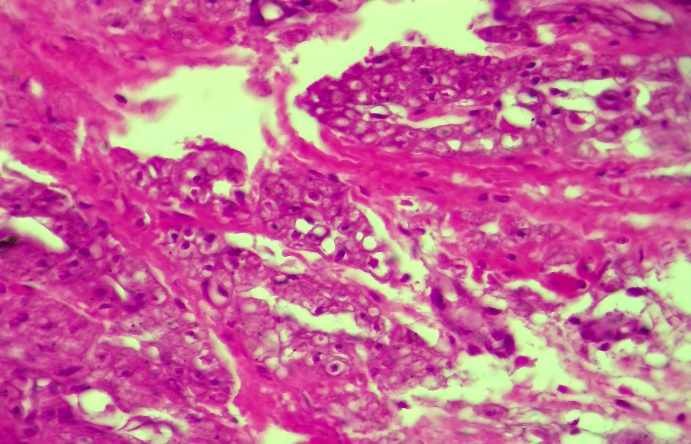
- The appearance of the congenital defect of the interventricular wall of the heart in the 3–8th week of the embryonic period depends on the pathological factors affecting the mother’s organism. Cardiomyogenesis begins in the 3rd week of the embryonic period and takes place from the accumulation of mesodermal cells of the visceral sheet of the mesoderm. The visceral sheet of the mesoderm is called the myocardial plate because it is located close to the tubes that turn into the heart cavity. The endocardium is formed from the mesenchymal tissue present on the inner surface of the tubules. In the 4th week of embryogenesis, myofibrils appear in the cells of the myocardial plates, and the synchronous contraction of muscle cells begins. Desmosomes appear in areas where the plasmolemmas of myoblasts are connected to each other.Later, the myocardium grows and thickens due to polyploidization of cardiomyocyte nuclei and hypertrophy due to the increase in the weight of hyaloplasm, cell regeneration, which continues with an increase in the number of cellular structures. The processes of polyploidization and hypertrophy provide an increase in volume of the myocardium and compensate for the burden on the heart.Based on the above reasoning, the defects that appear in the walls of the heart correspond to the period of myocardium formation and differentiation in 3–8 weeks of embryogenesis. Defects appear due to the influence of metabolites of various drugs from the mother’s organism and the effect of viral infection on the embryo, including the histogenesis and organogenesis of the heart embryogenesis, which is damaged and incompletely organized due to injury.Microscopic examination of a piece of tissue taken from the edges of a congenital defect of the interventricular wall of the heart muscle showed that a thin connective tissue layer appeared directly on the surface layer, and its surface was covered with a single–layer endothelium. It is observed that the transversely extending muscle bundles located under it are located in different directions, including in the area under the connective tissue membrane on the surface of the tumor, although the muscle fibers are arranged in a circular pattern along the hole–defect wall (Fig. 1), connective tissue bundles have grown between the muscle fibers. It is determined that the muscle fibers in the areas far from the hole–defect have formed tufts of different thickness and they are mainly located in the transverse direction.
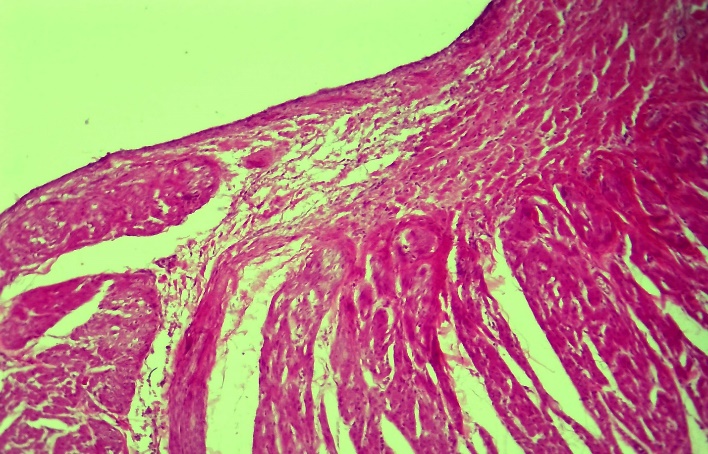 | Figure 1. The presence of a connective tissue membrane on the surface of the defect edge of the wall of the interventricular space of the heart, muscle bundles are located in different directions. Paint: G–E. Floor: 10x10 |
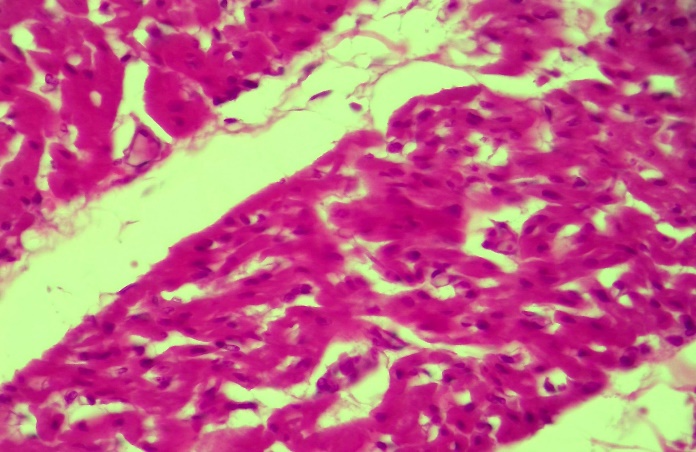
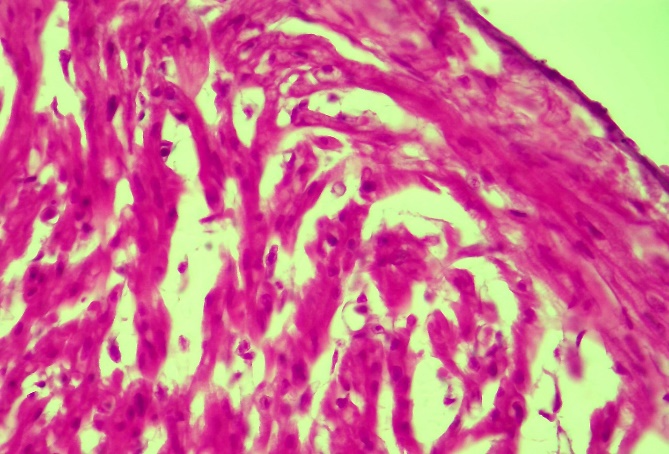 | Figure 2. There is a lack of cells in the connective tissue membrane on the surface of the defect of the wall of the interventricular space of the heart muscle, and the muscle bundles are narrowed due to swelling. Paint: G–E. Floor: 10x40 |
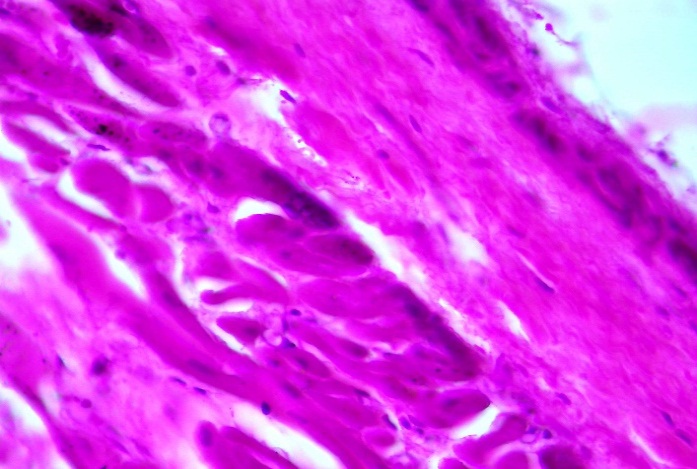 | Figure 3. Endothelial cells proliferated on the surface of the defect of the interventricular wall of the heart ventricles, the connective tissue membrane turned into fibrous tissue, and muscle fibers became hypertrophied. Paint: G–E. Floor: 10x40 |
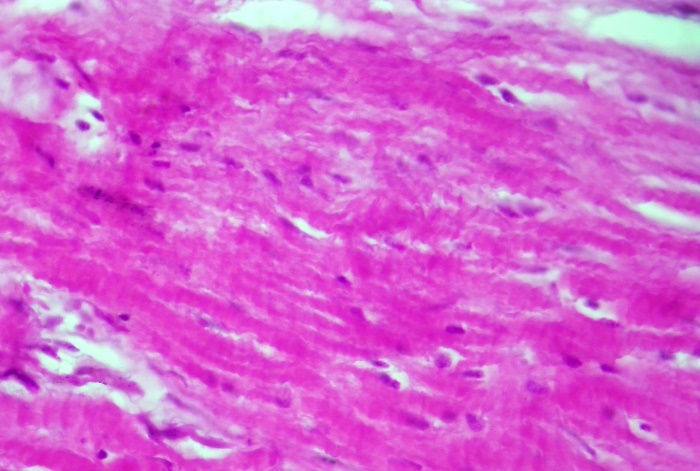 | Figure 4. Some of myocardium, muscle fibers and cardiomyocytes with congenital defects have undergone dystrophy, others hypertrophy. Paint: G–E. Floor: 10x40 |
 | Figure 5. Myocardium with a congenital defect, irregular arrangement of muscle bundles, the presence of fibrous tissue bundles between them, and the development of fatty dystrophy in cardiomyocytes. Paint: G–E. Floor: 10x40 |
 | Figure 6. Interventricular wall myocardium, from the histogenesis of muscle groups, their irregular arrangement. Paint: G-E. Floor: 10x40 |
5. Conclusions
- A thin rough fibrous connective tissue and endothelium appeared on the surface of the congenital defect of the wall muscle part of the heart ventricles, on its surface, fibrous tissue bundles spread around the interstitial tissue of the muscle fibers, transversely extending muscle fibers are located in different directions.The morphogenesis of the appearance of a congenital defect in the wall of the interventricular space of the heart consists in the fact that in the 3–4th week of the embryonic period, the mesodermal cells released from the visceral sheet of the mesoderm, where cardiomyogenesis takes place, accumulate less due to injury, and their transformation into muscle cells fails, and a certain part of the myocardium remains empty without development. and is born as a defect.During the development of a congenital defect in the wall of the interventricular space of the heart, a number of histological defects and deformations are preserved in the myocardial muscle tissue due to the violation of histogenesis and incomplete formation and differentiation of muscle cells in the preserved muscle tissue of this wall.