-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(9): 1002-1005
doi:10.5923/j.ajmms.20221209.32
Received: Sep. 3, 2022; Accepted: Sep. 23, 2022; Published: Sep. 29, 2022

Analysis of Commission Forensic Examinations Related to the Provision of Medical Care to Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZaynitdin Asamitdinovich Giyasov1, Mashrabjon Abdubakievich Dehkanov2, Sarvar Abduazimovich Hakimov3
1Doctor of Medical Sciences, Professor, Tashkent Medical Academy, Uzbekistan
2Expert, Andijan Branch of the Republican Scientific and Practical Center for Forensic Medicine
3Candidate of Medical Sciences, Senior Teacher, Tashkent Medical Academy, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In 2012–2021, the materials of a commission of forensic expertise related to the provision of medical assistance to children were examined in three regions. Two–thirds of cases with defects in health care were related to infants. Pediatricians, general practitioners, neonatologists and paramedical staff in outpatient institutions are more likely to be deficient. More than half of the defects had a diagnostic hue, more often in the form of rejection of the underlying pathology. A significant part of the defects were due to subjective reasons, mainly due to neglect of the patient. Many defects have seriously affected the outcome, creating a tendency for Death to surface, or directly leading to death.
Keywords: Commissioned forensic medical expertise, Children’s medical care, Ambulatory institutions, Medical care defects, Rural medical centers
Cite this paper: Zaynitdin Asamitdinovich Giyasov, Mashrabjon Abdubakievich Dehkanov, Sarvar Abduazimovich Hakimov, Analysis of Commission Forensic Examinations Related to the Provision of Medical Care to Children, American Journal of Medicine and Medical Sciences, Vol. 12 No. 9, 2022, pp. 1002-1005. doi: 10.5923/j.ajmms.20221209.32.
Article Outline
1. Introduction
- Relevance of the topic. Ensuring that children receive quality health care and improving the health of the younger generation is one of the main tasks of the health system. The issue of timely, full, high–quality medical care for children is devoted to a number of studies of specialists from different regions. (D.O.Ivanov et al., 2017; S.S.A.Iskandar, I.S.Isaev, 2018; T.M.Mekari et al., 2017).The simplest and most effective way to improve the quality of medical care is to identify medical care defects (MCD) and develop targeted measures to eliminate them based on a comprehensive analysis. (A.A. Baranov et al., 2015; V.J. Gawron et al., 2016). In this regard, the commission’s forensic-medical examinations (CFME) conducted in connection with professional offenses of medical personnel (POMP) have a special place. The main goal of this special practice is to help in the legal evaluation of the provided medical care, and the actions of medical personnel are thoroughly studied by the commission of experts. (A.V. Kovalev, A.A. Martemyanova, 2015). At this point, it should be noted that the materials of the CFME held in Uzbekistan on the subject of POMP have not been sufficiently studied by experts (2) (Z.A. Giyasov and others, 2019).The aim of the study is an expert assessment of defects in the provision of medical assistance to children on the basis of CFME materials.
2. Materials and Research Methods
- In 2012–2021, the subject of study was materials CFME, conducted in the Andijan, Namangan and Fergana regions in connection with the provision of medical assistance to children. During the years of the study, 364 surveys conducted in three regions revealed deficiencies in the provision of medical care to children, and the records of these surveys were thoroughly analysed. The expert commission, in accordance with the requirements of existing manuals and rules, includes clinicians–specialists in the field. Recommendations for modification of the classification, which took into account the specifics of medical care for children, were examined. In this connection, attention was paid to such aspects as the profession of the medical practitioner who allowed the defect and, in addition to the medical institution, the nature of the defects, the causes of the occurrence and the degree of influence on the final result. The records of the previous service inspections on the current situation in the case file were also analyzed. The collected database was marked with numerical codes on the basis of a special program and was statistically processed accordingly.
3. Results of the Study and Their Discussion
- A total of 419 MCD were identified in the 364 CFME mentioned above (in some cases there were 2 or more defects). In the period of the study, it was noted that over the past five years these cases have decreased significantly, both in absolute and relative terms.According to the analysis, more boys (38.7 per cent and 61.3 per cent respectively) were treated with disabilities than girls. When CFME materials were examined for age groups of children, two thirds of these cases were related to the care of infants, 17.3 per cent of which were neonatal. Children of school age accounted for 14.3 per cent (photo 1).
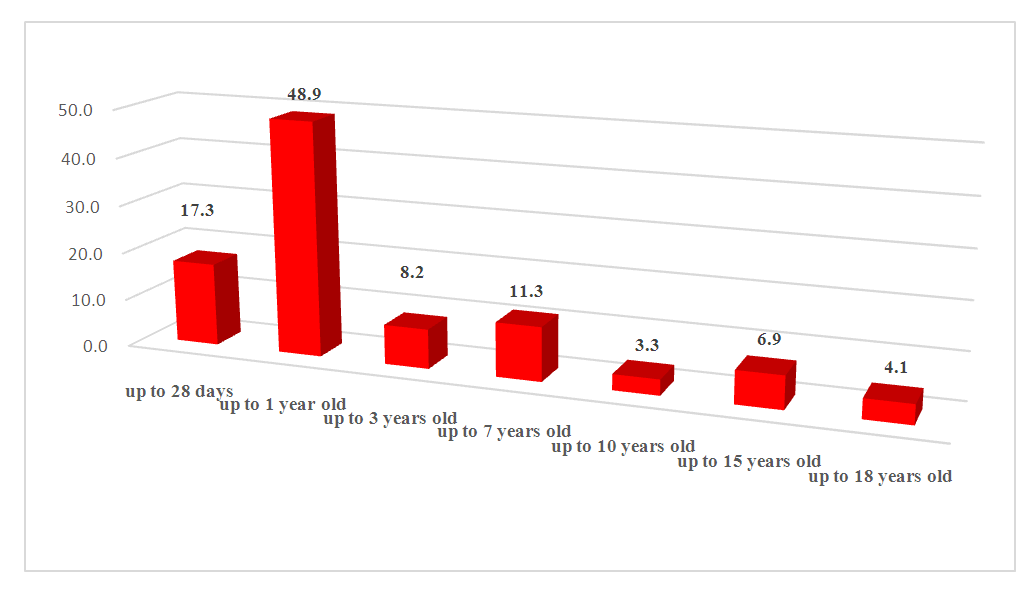 | Photo 1. Age distribution of observations |
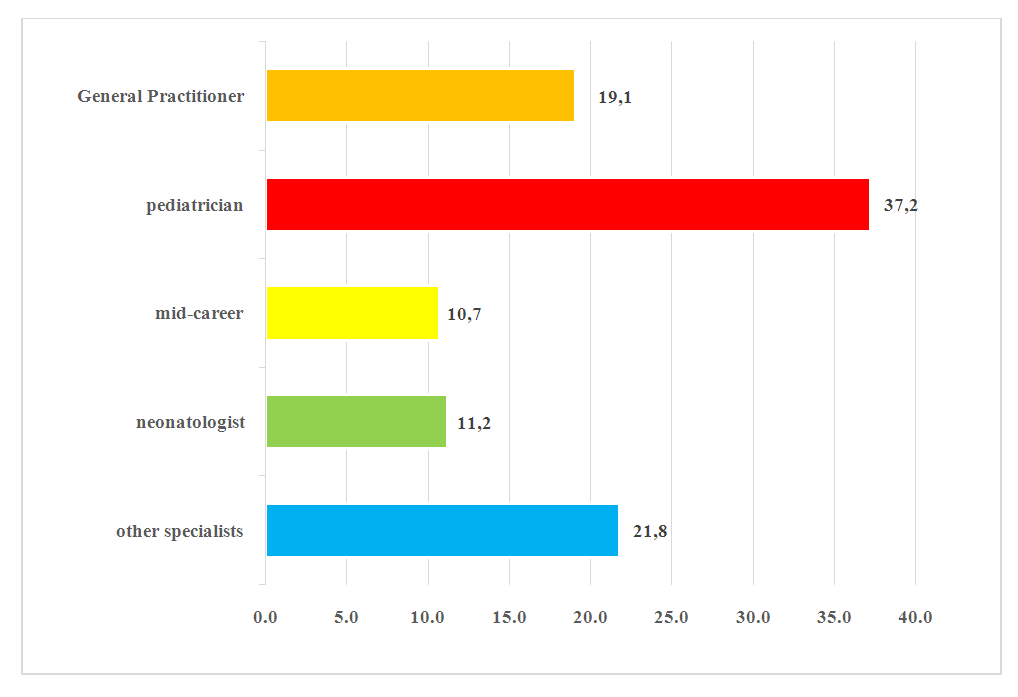 | Photo 2. Medical personnel in the specialties section |
|
|
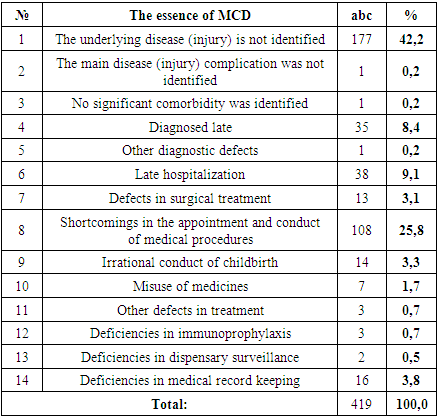
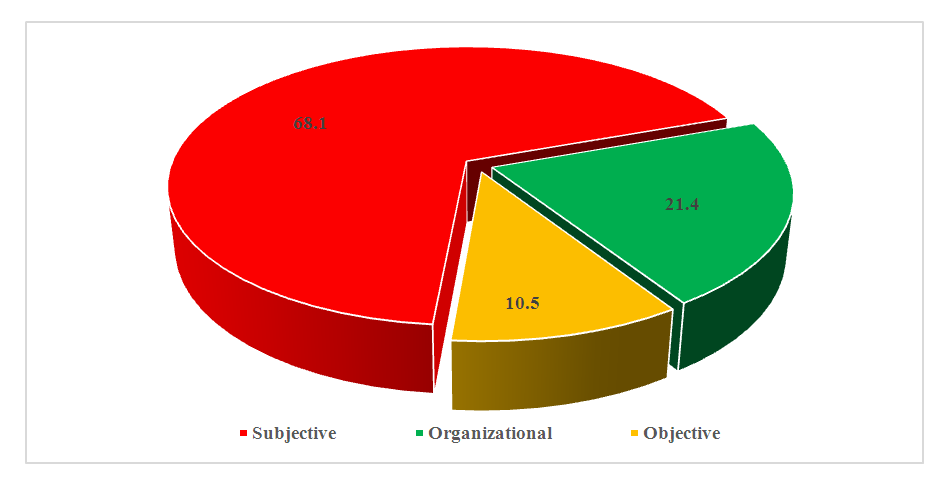 | Photo 3. Groups of causes of defects |
4. Conclusions
- Based on a comprehensive analysis of CFME materials related to the provision of medical care to children, the following conclusions can be drawn:1. Two thirds of cases in which defects are detected in the CFMEs are related to the care of infants, a quarter of which are neonatal.2. Defects were mainly attributed to paediatricians, general practitioners, neonatologists and nurses, more often in outpatient institutions.3. More than half of the MCD was associated with the diagnostic process, most of which were organized due to the absence of the underlying disease.4. 68.1% of the defects were due to subjective reasons, mainly due to neglect of patients by medical personnel. Based on 21.4% of the MCD, there were organizational reasons.5. Of the deficiencies in medical care, 71.9 per cent had a serious impact on the end result, most of which were predisposed to death.6. In improving the quality of health care, children should take into account the analysis of survey materials.