-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(9): 963-969
doi:10.5923/j.ajmms.20221209.24
Received: Sep. 10, 2022; Accepted: Sep. 20, 2022; Published: Sep. 23, 2022

Forensic Aspects of Fatal Outcomes of Combined Trauma to the Structures of the Head, Chest and Abdomen
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIndianov S. I.1, Umarov A. S.2
1Deputy Head of the Republican Scientific and Practical Center for Forensic Medical Examination, Uzbekistan
2Research Candidate of the Department of Forensic Medicine of the Samarkand State Medical University, Uzbekistan
Correspondence to: Indianov S. I., Deputy Head of the Republican Scientific and Practical Center for Forensic Medical Examination, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To improve the forensic expertise of fatal outcomes of combined trauma to the structures of the head, chest, and abdomen, the data of medical records, the results of laboratory and additional studies, as well as the conclusions of the forensic expertise of cadavers, were studied and analyzed, in respect of 434 persons with combined trauma received from medical institutions (hospitals). It is noted that in clinical practice, violations of the rules for maintaining medical records are most often allowed, especially in cases of bodily injury. At the same time, the algorithm for describing injuries on the body of victims does not meet the generally accepted medical criteria, which in the process of the forensic expertise does not allow to give answers to the questions posed by the judicial and investigative bodies on establishing the mechanism, prescription, severity of injuries. manifestations of the thanatogenesis of traumatic illness are recorded. Morphological manifestations of complications of ventilation, infusion-perfusion therapy, as well as critical and terminal conditions are not detected. Changes and complications caused by diagnostic, resuscitation, and surgical procedures at different stages of medical care for victims are not fully taken into account. A number of recommendations for improving the forensic expertise process of corpses of persons with combined trauma coming from hospitals are given. It is emphasized that the lethal outcome of combined trauma in some cases may be due to complications of diagnostic, and surgical interventions, as well as defects allowed in the process of diagnosis and treatment, or exacerbations of chronic somatic diseases.
Keywords: Combined trauma, Head, Chest, Abdomen, Mortality, Examination, Improvement
Cite this paper: Indianov S. I., Umarov A. S., Forensic Aspects of Fatal Outcomes of Combined Trauma to the Structures of the Head, Chest and Abdomen, American Journal of Medicine and Medical Sciences, Vol. 12 No. 9, 2022, pp. 963-969. doi: 10.5923/j.ajmms.20221209.24.
Article Outline
1. Actuality of the Problem
- In the context of a steady increase in combined trauma (CT) associated with an increase in the number of road traffic accidents (accidents) and catatraumas, effective methods of early diagnosis and principles of treatment of patients with polytrauma are being developed. [2,3,8,19,22,26], however, to date, the mortality rate from ct remains quite high, reaching up to 80% at the prehospital and up to 60% at the hospital stage. The effectiveness of medical care for victims with CT in the prehospital, resuscitation, profile-clinical and rehabilitation periods, to a certain extent, depends on the severity of the injury and the timeliness of the organization of emergency care. It is believed that when providing qualified assistance during the feathers 60 minutes after the injury, there is a greater chance of saving the lives of the victims, while the mortality rate can reach up to 10%. At the same time, with an increase in the period of provision of such assistance to 8 hours, the mortality rate can increase to 75% [41,46]. In forensic terms, CT is of interest in terms of establishing the nature, cause of death, thanatogenesis, qualification of the severity and determination of the mechanical genesis of the injury, as well as the identification and evaluation of defects in the provision of medical care at various stages of treatment of victims. Establishing the cause of death and thanatogenesis of CT, especially after carrying out therapeutic and diagnostic measures, present significant difficulties. Death from CT can be associated not only with trauma and its complications, but can also be associated with resuscitation, surgical complications, defects made in the process of diagnosis and treatment, as well as exacerbations of somatic diseases. Therefore, the process of studying the corpses of persons who died from CT, after surgery or other therapeutic and diagnostic measures requires a special methodological approach. Before starting the study of the corpse, it is necessary to study the medical history very carefully, but the records in the medical history require a critical attitude since the data presented may be insufficient (for example, descriptions of injuries) or exaggerations (unreasonable diagnosis). These and other aspects of CT for solving the problems of forensic expertise (FE) have not been studied and investigated enough [28,33,36].
2. The Purpose of the Study
- The purpose of the study was the improvement of FE deaths of combined trauma to the structures of the head, chest and abdomen.
3. Materials and Methods of Research
- The following data were studied and analyzed: the data of medical records, the results of laboratory and additional studies, as well as the conclusions of the FE of corpses, in respect of 434 persons aged 7 to 78 years with CT received from medical and prophylactic institutions (MPI). Most of the dead persons from CT were men (76%) of the most employment age - from 18 to 60 years (69.8%). FE corpses were carried out by State Experts for the period 2015-2021 in the regional branches of the Republican Specialized Scientific-Practical Center for Emergency Medicine under the Ministry of Health of the Republic of Uzbekistan under standards A-1, (Order of the Ministry of Health of the Republic of Uzbekistan No. 82 of 04.03 2015).Information about the circumstances of the injury was established according to the data of the decisions on the appointment of the FE, copies of the protocols, catamnesis, as well as medical records. It was found that the origins of CT were due to: intra-salon car injury (33%), collisions of pedestrians with moving vehicles (51.4%), moto- and bicycle trauma (6.7%), falling from a height (6.5%), jumping into a pond (0.5%), crashing under massive objects (4), exposure to blunt objects (1.1%). It can be seen that the origin of CT was dominated by road accidents - (91.1%). Victims with CT were in hospitals of central district hospitals (43.5%), city hospitals (14.5%), regional branches of the Republican Specialized Scientific-Practical Center for Emergency Medicine (36.9%), multidisciplinary regional hospitals (1.2%), and other medical institutions (3.9%). Thus, in most cases, the victims were in the nearest specialized hospitals (96.1%). In 43.6% of cases, victims with CT were in hospitals for up to 1 day, 14.2% - 1-3 days, 15.6% - 3-5 days and 8.06% - for 6 to 10 days. In 5.6% of cases, the exact period of stay of victims in hospitals has not been established.A significant number of classifications of CT (polytrauma) are given in the literature, but to date, there is no single unified classification covering all aspects of CT. According to several authors, the clinical and anatomical classification of V.A. Sokolov et al. (2006) is the most optimal for systematizing the clinical and pathomorphological aspects of CT, according to which all types of CT can be attributed to the following groups: 1. – combined craniocerebral trauma; 2-combined spinal cord injury; 3- combined chest trauma; 4- combined trauma to the abdomen and organs of the retroperitoneal space; 5-combined injury of the musculoskeletal system; 6-combined injury with two or more severe injuries; 7-combined injury without severe injury. This classification was taken by us as a basis in the process of systematization of CT cases. It was revealed that on the body of the dead, the CT of the head, chest, and abdomen (13.8%). The CT of the head and chest (13.5%), the CT of the head (12.2%), and the CT of the head, chest, abdomen, and upper extremities (6.4%) prevailed.Quantification of the data obtained from the medical records and conclusions of the FE was carried out according to a 5.0 point system, in which indicators from 0 to 5 indicated the following data: 0- lack of information; 1- very superficial information; 2- superficial information; 3- insufficient information; 4- not quite complete information; 5- full information. Within the framework of variational statistics, the criterion for the reliability of damage indicators - (t), their minimum error (m), and the reliability of differences (p)indicator to it were determined.
4. Research Results and Their Discussion
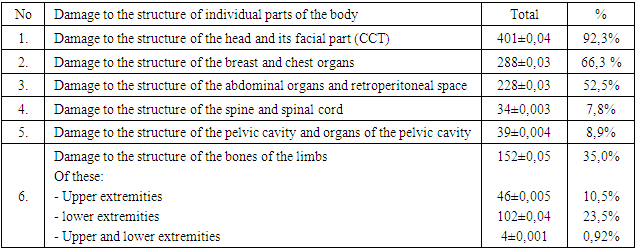
- It was established that the following types of damage to the structure of individual parts of the body took place in the composition of the CT (Table No.1).
|
5. Discussion
- Combined trauma as a result of blunt mechanical factors continues to have an adverse effect on the health indicators of people in different countries and the demographic situation as a whole. Along with the growth of cardiovascular and oncological diseases, there is a steady increase in injuries around the world. There is also a high frequency of disability (25-45%) and deaths of the population (40-60%) as a result of combined and multiple injuries. In this regard, injuries are currently becoming a highly urgent social, medical and economic problem [2,8,24,40].According to leading neurosurgeons in the structure of modern CT, damage to the structure of the skull and brain is diagnosed in at least 75% of the victims. CCT worldwide remains to date the most pressing medical, social and economic problem due to its prevalence and severity of its consequences. In severe types of CCT, structural and functional damage to the brain at the molecular, subcellular, cellular, tissue and organ levels is formed primarily, which leads to disorders of the central regulation of all systems in the body. There are violations of cerebral circulation, cerebrospinal fluid, the function of the hypothalamus, the pituitary-adrenal system and lesions of the blood-brain barrier are formed. As a result, edema, swelling of the brain and dislocation syndrome develop with infringement of the brain and cerebellum in the occipital opening and, thereby, blood circulation, cerebrospinal fluid regulation, metabolism and functional activity of the brain deteriorate sharply. Modern methods of radiant diagnostics, in particular diffuse-tensor (DT) MRI, allow in vi to quantify the architectonics of white matter and obtain reliable information even with diffuse-axonal damage (DAP). It is emphasized that the corpus callosum is the most vulnerable in the conditions of the DAP. Combined damage to the structure of the breast and organs of the chest cavity is one of the most commonly observed injuries, which in the vast majority of cases are accompanied by traumatic, pleuropulmonary shock, manifestations of hemo and pneumothorax. These conditions, along with trauma to the structure of other parts of the body, most often the head and abdomen, are the direct cause of death of victims in the prehospital stage. According to a number of authors, damage to the structure of the breast, among the causes of mortality, occupy one of the leading places, second only to CCT [12,42]. As part of CT, closed injuries to the structure of the chest and chest cavity organs are observed 9 times more often than open (penetrating and non-penetrating) injuries that can be without damage (71.8%) or accompanied by damage to internal organs (28.2%). The nature of the damage can vary from ordinary bruises to gross injuries - to the complete separation of internal organs, accompanied by massive blood loss. The main causes of chest injuries (up to 97.3%) are accidents and fall from a height. Life-threatening complications of chest injuries requiring emergency care include cardiac tamponade; massive hemothorax; tense pneumothorax; open pneumothorax; development of the costal valve; rupture of the diaphragm [53]. It is emphasized that with lesions of the structure of the chest and organs of the chest cavity, pulmonary complications in the early and late periods of traumatic illness are the main cause of mortality of patients. The number of such complications in multiple injuries reaches up to 86%, of which about 20% of cases of pulmonary complications are detected a few days after the injury [39,41,42]. In an earlier period of injury, pulmonary complications develop as a result of lung contusion, hemo and pneumothorax, aspiration of blood into the respiratory tract, embolism of fats and atelectasis. In the long-term period of injury, the causes of pulmonary complications are infectious complications (purulent tracheobronchitis, croupous pneumonia, bronchopneumonia, hemopleurisis, pleural empyema, etc.) [49,51].It was revealed that 50-60% of victims with breast CT have damage to the lungs and tracheo-bronchial structures, which are the most common causes of death of the victims [44,45]. With a closed chest injury, tracheal ruptures in CT are observed from about 1.4 to 5.0% of cases [50]. At the same time, large bronchi are most often damaged than trachea. Damage to the structure of the trachea and bronchi in CT is extremely dangerous, posing a threat to the life of the patient. Unfortunately, in the process of FE of cadavers with CT, damage to these structures often remains unrecognized due to an inadequate study of the structures of the organs of the mediastinum and neck. In this regard, there is a need for a more detailed analysis of the literature data on the features of the lesion of the structures of the trachea and bronchi in different types of blunt trauma. We believe that these data will undoubtedly increase the reliability and validity of expert studies of cases of trauma to the structure of the chest and organs of the chest cavity. According to specialists in thoracic surgery, the localization and nature of the injury to the trachea and bronchi is important for emergency care and the choice of treatment method. A distinction is made between closed and open trauma to the trachea. By localization, the following are damaged: cervical, thoracic parts, and bifurcation of the trachea; by nature, longitudinal, transverse, partial and complete damage are distinguished. In addition, a multifocal injury is distinguished, in which the lesions cover several parts of the trachea. The cervical part of the trachea is a less protected area of it, so ruptures of this department are often observed. However, injuries to the thoracic region pose the greatest danger and stopping them is more difficult. The main bronchi are also damaged frequently [5]. Damage to the structure of the trachea and bronchi is often combined with traumatization of the venous and arterial vessels of the esophagus, which significantly aggravates the course of the process and is complicated by massive blood loss. In addition, such injuries may be accompanied by aspiration into the respiratory tract with the development of asphyxia. These circumstances require immediate isolation of the tracheobronchial tree from the source of bleeding and restoration of ventilation of the lungs when assisting the victims.With an injury to the cervical spine of the trachea, damage to different parts of the larynx is also possible, which may be accompanied by trauma to the esophagus and the recurrent (laryngeal) nerve. Similar conditions are often noted in drivers and passengers with auto trauma as a result of flexion and extensor movements of the head and neck. These injuries require the imposition of a tracheostomy and the restoration of the integrity of the esophagus. Injuries to the trachea can be combined with a contusion of the lungs. With a chest injury with rib fractures, the lesion of the lung tissue is complicated by respiratory failure - the "gas syndrome", in which intubation of the trachea may not be effective. Treatment of small ruptures of the trachea and bronchi can be conservative. However, with significant ruptures of the trachea, especially with lesions of its thoracic region, surgical intervention is indicated [23].Analysis of the conclusions of the FE of cadavers with CT shows that in the process of studying damage to the organs of the chest cavity, expert doctors usually do not pay attention to the presence of damage to the structure of the trachea, bronchi and esophagus, they are limited only to describing the condition of the lungs, heart and diaphragm. As can be seen from the above, the mechanism of injury to the structure of the trachea, bronchi and esophagus has its characteristics. They are very life-threatening injuries and are often the direct cause of death of victims. Damage to the structure of the abdominal organs, with different types of mechanical trauma, is 21-25% and does not tend to decrease [27,29]. At the same time, intestinal damage ranges from 6.3 to 38.5%, and mortality reaches up to 12-24% [4,7,17], which are the most common cause of peritonitis. With traumatic effects from the abdominal organs, the small intestine is most often damaged, then the liver and spleen [13,47]. The frequency of liver damage in abdominal injuries ranges from 56 to 66.8% [18,37,52]; and in 37-45% of cases there are complications in the postoperative period [1,9,19,38], the mortality rate of patients in the postoperative period reaches 30-36%, and with LIVER CT - 39-44% [1]. Clinical and morphological classification of liver damage according to E. Moore et al. [30] provides for their division into the following degrees of severity: I - subcapsular accumulation of blood more than 10% of the area, rupture of the parenchyma up to e 1 cm, not bleeding; II - hemorrhage with a subcapsular within 10-50% of the area, tissue rupture up to 2.0 cm deep to 3 cm, up to 10 cm long with bleeding; III - hemorrhages under capsule with an area of about 50% rupture of the parenchyma over 3 cm, bleeding; IV - subcapsular hemorrhage with damage to the parenchyma in the range of 25-50%, occupying up to 3 segments; V - damage to more than 50% of the parenchyma, occupying at least 3 segments, covering the vascular system; VI - liver ruptures and vascular injuries. According to Muller G., Little K. (2001), the frequency of occurrence of various degrees of liver damage is: I - 32.2%; II - 33,1%; III -22,2%; IV - 9,6%; V - 2.9%, VI - the degree was not noted [32].More dangerous are crushing of the liver parenchyma, accompanied by intra-abdominal bleeding, mortality can reach up to 34-35% [6,9]. Such conditions require immediate surgical intervention for injuries. The delay of the operation by more than 6 hours, associated with diagnostic and tactical errors, can cause death in victims with trauma to the abdominal organs [14]. According to different authors, mortality with isolated liver damage reaches up to 15%, and with combined abdominal trauma -50.0-80.0% [10,11,16,19, 21,35,45,54].The described degree of liver damage is more acceptable for forensic research. However, when analyzing a fairly large number of FE conclusions of cadavers with CT, we were not able to identify the presence of detailed and systematic descriptions of liver damage on this principle. In our opinion, compliance with the principles for determining the degree of damage to the liver and spleen in the process of FE cadavers will undoubtedly improve the quality and validity of studies. In addition, identifying the degree of organ damage can help to identify defects in the medical care of victims, in cases of death of patients in hospitals. To improve the quality of the examinations carried out and the solution of the above tasks with CT, a full-fledged qualitative study and description of damage to organs and tissues is required in the prescribed manner: with CCT - the exact localization and directions of fractures, localization, volume, source of epi - and subdural hematomas, subarachnoid hemorrhages. It is necessary to examine the brain by special methods. Determine the topography, the area of subarachnoid hemorrhages and foci of brain contusions. It is necessary to conduct a forensic histological examination of the structure of the brain from the area of bruises and outside the areas of bruises; in case of damage to the chest and chest cavity organs, it is mandatory to conduct a test for pneumothorax, preferably an X-ray or ultrasound of the chest before the opening. Very carefully examine and fully describe the states of the plates at the edges of rib fractures, indicating the exact localization of fractures along anatomical lines, determining the presence of damage to the structure of soft tissues in the fracture area; for the study of spinal cord injuries, the most acceptable is the method of A.A. Solokhin (1968). Taking into account the complexity of this method, X-ray of the spinal column, and, if possible, computed tomography, is acceptable for establishing the localization, type, and nature of vertebral fractures and damage to their structures. In the process of FE of corpses with spinal trauma, it is possible to conduct mechanical cleaning of the area of damage to CT soft tissues, which significantly contributes to the study and description of traumatic changes in the vertebrae and their structures. The type and nature of vertebral fractures must be determined in accordance with clinical and anatomical classifications intended separately for the upper cervical, lower cervical and thoracic lumbar regions [Kotelnikova G.P., 2008]; in case of accidents and falls, it is mandatory to study the soft tissues of the back surface of the body in the prescribed manner. The nature of fractures of the bones of the pelvis and limbs should be determined by unified clinical and anatomical classifications; it is also necessary to improve the study and qualified description of injuries of soft tissues, and internal organs; in all cases, it is necessary to conduct forensic histological studies of the brain and internal organs using the methods of modern morphometry.
6. Conclusions
- 1. In the materials of forensic examination of cases of combined trauma, more than 1/3 (35.2%) of the corpses examined are considered. Combined trauma is dominated by CCT (46.9%) and trauma to more than 2 parts of the body, mainly the head, chest and limbs (22.2%). In 63.1% of cases, the death of victims of combined trauma occurs at the sites of injury, and in 36.9% of cases, death is observed in hospitals;2. The immediate causes of death of victims of combined trauma on the next day after the injury were: gross anatomical trauma of more than 2 parts, severe CCT, massive blood loss, traumatic and hemorrhagic shock, cervical-occipital trauma, and in some cases - cardiac tamponade, bilateral hemopneumothorax, pleuropulmonary shock, aspiration of blood in the respiratory tract; in an earlier period of CT (1-3 days), the cause of death of the victims was due to edema and dislocation of the brain, shock, fat embolism of the vessels of the brain and lungs; in a remote period (more than 3 to 8 days) of trauma - from purulent-septic complications, pulmonary embolism, multiple organ failure; 3. In the process of examination and treatment of patients with combined trauma, violations of the rules for maintaining medical records are most often committed, while the algorithm for describing injuries on the body of victims does not meet generally accepted medical criteria, that in the process of FE corpses do not allow a reliable answer to the questions posed by the judicial and investigative bodies, on establishing the nature, instruments of injury, mechanism, and prescription; Defects in the diagnosis and treatment of combined trauma can be masked by the severity of the injury. However, in the early post-traumatic period of trauma at the pre- and hospital stages, diagnostic defects are often allowed - the main injury and its complications are not detected on time, or concomitant (competing) pathologies are not established, and therefore insufficient or inadequate treatment is carried out. In the late post-traumatic period of injury, defects are reduced to underestimation of the severity of the victim, inadequate treatment of the injury and their complications;4. The descriptive part of the conclusions of the FE of corpses of persons with combined trauma received from hospitals, regardless of the duration of the injury, is described almost in the same way, manifestations of thanatogenesis of traumatic illness are not recorded. Morphological manifestations of complications of ventilation, infusion-perfusion therapy, as well as critical, terminal conditions are not detected. In this regard, according to these conclusions, it is impossible to reliably and reasonably establish the mechanism and thanatogenesis of combined trauma. The conclusions of the examinations also do not fully take into account the changes and complications caused by diagnostic, resuscitation, and surgical procedures at different stages of medical care for the victims. 5. Advances in modern surgery in close connection with the improvement of anesthesia methods have led to a sharp increase in surgical interventions, and this, in turn, has led to an increase in several intra- and postoperative complications, such as iatrogenic injuries of the trachea, esophagus associated with intubation, or complications of catheterizations and other procedures. Consequently, the lethal outcome can be associated not only with trauma and its complications, but can also be due to post-resuscitation, postoperative complications, defects made in the process of diagnosis and treatment, as well as exacerbations of chronic somatic processes. These data should be taken into account in the process of diagnosis and expert evaluation of the outcomes of combined injuries.