-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(8): 840-844
doi:10.5923/j.ajmms.20221208.16
Received: Jun. 23, 2022; Accepted: Aug. 10, 2022; Published: Aug. 25, 2022

Tuberculous Spondylitis: Differentiated Approach to the Diagnosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLZulfiya Makhmudova
Republican Specialized Scientific and Practical Medical Center of Tuberculosis and Pulmonology, Tashkent, Uzbekistan
Correspondence to: Zulfiya Makhmudova, Republican Specialized Scientific and Practical Medical Center of Tuberculosis and Pulmonology, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. The purpose of this study is to generalize the results of a complex clinical-laboratory, radiological and immunological study of patients with spinal tuberculosis. Materials and Methods. A comprehensive examination analysis was carried out in 192 patients with tuberculous spondylitis who were in the department of surgery for osteoarticular tuberculosis of the Republican Specialized Scientific and Practical Medical Center of Tuberculosis and Pulmonology in Tashkent, Uzbekistan. Results. Severe degrees of spinal disorders were found in 48.7% patients. Magnetic resonance imaging (MRI) and multi-slice spiral computed tomography (MSCT) allowestablishing the stage and activity of a specific process in the spine, as well as complications. Spinal column instability was detected in 143 (74.5%) patients, paravetebral abscesses in 116 (60.4%) patients, and epidural abscesses in 75 (39.0%) patients. Changes in immunological parameters in patients with spinal tuberculosis were associated both with impaired regulation of immunogenesis and with the direct influence of the immune system at various stages of the process. The detection of certain patterns of immune system disorders in patients with tuberculous lesions of the spine allowed us to make a differentiated approach to their treatment in order to increase the effectiveness of the treatment. Conclusions. It can be concluded that at present, tuberculosis of bones and joints, especially the spine, is detected in an advanced stage in 50-80% of cases and has a widespread and complicated character with profound anatomical and functional changes and the presence of severe spinal disorders in 48.7% patients in Uzbekistan. Regarding spondylitis, it is immensely important to make an accurate diagnosis based on the clinical presentations, laboratory, radiological and immunological findings and by periodic assessment of the response to treatment, which is essential in atypical cases.
Keywords: Extrapulmonary tuberculosis, Spondylitis, Neurology, Immunology
Cite this paper: Zulfiya Makhmudova, Tuberculous Spondylitis: Differentiated Approach to the Diagnosis, American Journal of Medicine and Medical Sciences, Vol. 12 No. 8, 2022, pp. 840-844. doi: 10.5923/j.ajmms.20221208.16.
1. Introduction
- Tuberculosis spondylitis or spinal tuberculosis has been known since ancient times. Hippocrates and Galen also mentioned this disease in their medical investigations. In 1779, the first detailed description of its main symptoms (hump and related paralysis) was given by the English surgeon PersivewellPott, who consequently named this disease in the English literature as “Pott`sdesease” [1].Tuberculous spondylitis is one of the most serious chronic infectious diseases caused by Micobacterium tuberculosis affecting the vertebral bodies, spinal cord and surrounding organs [2,3]. In addition, it is characterized by the formation of specific granuloma and progressive destruction of the bone, leading to severe organic and functional disorders of the affected skeleton. It also occurs much more often than it is registered. For instance, only a smaller part of the patients, suffering from tuberculous spondylitis, are actively and timely detected [4,5], and therefore some patients do not receive timely and correct treatment [6,7,8].In recent years, tuberculosis spondylitis or spinal tuberculosis has shown a considerable resurgence in not only developing countries, but also in developed ones, particularly among the immunosuppressed population, mainly as a consequence of higher human immunodeficiency virus (HIV) infection and immigration rates [9].This disease has become a serious challenge to the global community. Since a few decades, an inauspicious upward trend in the number of multidrug-resistant tuberculosis strains is observed in developing countries. Due to these reasons, currently, the disease continues to exist as a critical global public health menace [10]. The diagnosis of tuberculous spondylitis remains a clinical challenge despite all technological advances, since it depends on a high grade of clinical suspicion. In spite of the low reported mortality of tuberculous spondylitis, this condition is still associated with substantial clinical morbidity. Particularly, considerable delay in diagnosis may lead to irreversible neurological complications and severe skeletal deformities [11]. Moreover, the slow development of a specific process in the spine, unclear symptoms, and the long course of tuberculosis gradually turn the patient into a severely disabled person. A number of such patients are accumulating, their treatment and maintenance require material costs and hence, it all turns into a medical and social problem [8,12]. At the same time, thanks to the achievements of modern medicine (mainly surgery) in the Republic of Uzbekistan, all localizations and forms of tuberculous spondylitis are treatable [13,14].The spinal tuberculosis diagnosis, as a rule, is based on a comprehensive assessment of clinical manifestations, such as data from laboratory analyses and the results from radiological studies [7,15,16,17,18,19]. However, even with the presence of high-tech diagnostic methods, tuberculous spondylitis is still detected in 40% cases in the later stages, and common and complicated forms are found in 70% of adult patients [8,20,21,22].According to the number of researchers [6,7], the clinical and radiological data similarity of these borderline diseases leads to the fact that the majority of patients with nonspecific spine osteomyelitis are sent for treatment to specialized hospitals with a preliminary erroneous diagnosis of tuberculous spondylitis. At the same time, the authors note that the accumulated experience in the treatment of tuberculous spondylitis in TB hospitals can be used in the treatment of patients with non-specific inflammatory diseases of the spine [23,24]. The purpose of this study is to generalize the results of a complex clinical-laboratory, radiological and immunological study of patients with spinal tuberculosis.
2. Materials and Methods
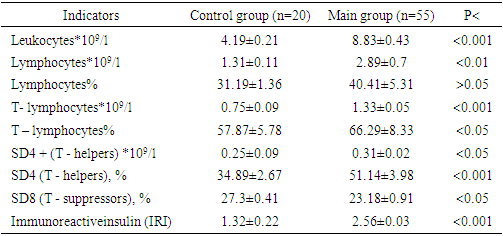
- A comprehensive examination analysis was carried out in 192 patients with tuberculous spondylitis who were in the department of surgery for osteoarticular tuberculosis of the Republican Specialized Scientific and Practical Medical Center of Tuberculosis and Pulmonology in Tashkent, Uzbekistan. The anamnesis, clinical and laboratory data (general analysis of blood, urine, biochemical research and a blood coagulogram), ECG, HPF, ultrasound of the abdominal cavity, pelvis and retroperitoneal space, as well as the pleural cavity were studied. Neurological status was assessed using the Frankelscale.Radiological examination was carried out using X-ray in the sagittal and frontal projections, and MRI of the affected segment. CT and MRI were performed according to indications for the differential diagnosis of the pathological process. The study was conducted on MRJ SYGNA HD/e (General Electric USA) apparatus with a capacity of 1.5 Tesla and MSCT (32 slices). MSCT and MRI examination were studied in sagittal, frontal and axial projections. The thickness of the tomographic section of MSCT was from 2 to 5 mm. Sputum, postoperative material, fistula contents, pus, punctate, pleural fluid were subjected to bacteriological examination. The methods of bacteriological research were performed using smear microscopy, Gene-Xpert/Rif molecular genetic analysis, HAIN test, culture study on solid Levenshtein-Jensen medium, followed by automated incubation and growing of mycobacterial cultures on MGYT-960 liquid medium using BACTEC-MGYT- apparatus 960, as well as by determining the sensitivity of mycobacterium tuberculosis to antibiotics. The immune status was studied in 100 patients using indicators of cellular and humoral immunity. Such study was based on determination the percentage of lymphocytes, the number of T - and B – lymphocytes, subpopulation of T - lymphocytes - T - helpers and T – suppressors. The phenotype of immunocompetent cells was determined using monoclonal antibodies CD3, CD4, CD8, CD25 and CD95 (manufactured by Sorbent-ZTD) according to the Aguiar et al. [25] method. The level of serum immunoglobulins in the secrets composition was determined by method of radiological immunodiffusion according to the Lighaam and Rispens [26] and Mancini G. et. al. [27] method using standard monospecific antisera which was received from NI Mechnikov Scientific Research Institute of Microbiology, Moscow.
3. Results and Discussions
- The age of patients ranged from 20 to 70 years old (average age - 42 years old): 102 men (53.1%) and 90 women (46.9%). Tuberculous spondylitis, detected for the first time, amounted to 144 (75.0%) patients, and previously registered in the dispensary - 48 (25.0%). By localization: the lumbar spine was affected in 70 (36.5%) patients, the lumbosacral in 40 (20.8%), the lumbar in 40 (20.8%), the thoracic in 22 (11.5%), cervicothoracic in 10 (5.2%) and cervical in 10 (5.2%) patients.A relatively frequent lesion of the lumbar, lumbar-sacral, and thoracolumbar spine was noted, which can be explained either by a heavy load, or trauma of a different nature (trigger): acute or chronic associated with a profession or anatomical-functional structure, massive bleeding, etc.Injuries of a different nature, and orthopedic changes (scoliosis of varying degrees) and chronic concomitant diseases are triggers in the pathogenesis of tuberculosis of bones and joints with a premorbid background. Concomitant diseases were found in 144 (75.0%) patients. A cardiovascular system disorders were found in 89 (46.4%) patients, anemia of a different nature in 69 (35.9%), hepatobiliary system in 29 (15.1%), diseases of the urinary system and genitals in 13 (6.7%), and diabetes mellitus in 13 (6.8%) patients.A generalized form of spinal tuberculosis with lung damage was detected in 24 (12.5%) patients. Mycobacterium tuberculosis was revealed in the sputum of these 11 (45.8%) patients.The inflammatory process was accompanied by severe intoxication syndrome: an increase in body temperature (before febrile illness) was observed in 85 (44.3%) patients, weakness and sweating in 53 (27.6%), loss of appetite in 125 (65.1%), and weight loss more than 10 kg in 104 (54.2%) patients.The most formidable complication of tuberculous spondylitis is spinal cord compression, leading to paresis, paralysis of the extremities, impaired function of the pelvic organs, abdominal cavity, etc. Neurological complications of a different nature were revealed in 154 (80.2%) patients.
|

|
4. Conclusions
- 1. At present, tuberculosis of bones and joints, especially the spine, is detected in an advanced stage in 50-80% of cases and has a widespread and complicated character with profound anatomical and functional changes and the presence of severe spinal disorders in 48.7% patients in Uzbekistan.2. MRI and MSCT allow establishing the stage and activity of a specific process in the spine, as well as complications. Spinal column instability was detected in 143 (74.5%) patients, paravetebral abscesses in 116 (60.4%) patients, and epidural abscesses in 75 (39.0%) patients. 3. Changes in immunological parameters in patients with spinal tuberculosis were associated both with impaired regulation of immunogenesis and with the direct influence of the immune system at various stages of the process. The detection of certain patterns of immune system disorders in patients with tuberculous lesions of the spine allowed us to make a differentiated approach to their treatment in order to increase the effectiveness of the treatment. 4. It is immensely important to make an accurate diagnosis based on the clinical presentations, laboratory, radiological and immunological findings and by periodic assessment of the response to treatment, which is essential in atypical cases.