-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(8): 832-835
doi:10.5923/j.ajmms.20221208.14
Received: Apr. 23, 2022; Accepted: Jul. 25, 2022; Published: Aug. 23, 2022

Surgical Treatment of Patients with Heel Spurs in a Minimally Invasive and Highly Effective Way
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIrismetov M. E., Shokirov A. M., Tadjinazarov M. B.
Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics
Correspondence to: Tadjinazarov M. B., Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Purpose of the study. To improve the results of surgical treatment of heel spurs by using endoscopic methods, allowing early activation and rehabilitation of patients. Material and methods. Our center studied 38 patients aged 26 to 60 years, 20 men and 18 women, suffering from heel spurs. All patients were treated between March 2018 and May 2021. Results. We studied the results at 3 and 6 months in all patients. Long-term results were studied in 27 patients. Good results were noted in 36 (94.7%) patients, satisfactory in 2 (5.3%) patients. In the postoperative period, immobilization was maintained until the sutures were removed, the load was resolved after 3 weeks. after surgery, depending on the size of the calcaneal osteophyte defect. Conclusion. reduced trauma, increased efficiency of diagnosis and surgical treatment of calcaneal osteophyte, early activation and rehabilitation of patients.
Keywords: Heel spur, Plantar fasciotomy, Endoscopic method, Medial and lateral approach
Cite this paper: Irismetov M. E., Shokirov A. M., Tadjinazarov M. B., Surgical Treatment of Patients with Heel Spurs in a Minimally Invasive and Highly Effective Way, American Journal of Medicine and Medical Sciences, Vol. 12 No. 8, 2022, pp. 832-835. doi: 10.5923/j.ajmms.20221208.14.
Article Outline
1. Introduction
- Calcaneal spur syndrome is one of the most common and potentially devastating foot injuries. A calcaneal spur occurs when a bony osteophyte forms on the heel bone. They can be located on the back of the heel or under the sole. The relationship between spur formation, the calcaneal tubercle, and the calcaneus internal musculature results in a permanent stretching effect on the plantar fascia, which further leads to an inflammatory response [8]. It is believed that calcaneal spurs are a common cause of heel pain, however some cases are asymptomatic, with most studies reporting up to 16% and Barthold reporting 30% of cases [9]. Kuyucu et al. investigated the association of calcaneal spur length with plantar fasciitis and they reported that calcaneal spur size is an important factor in terms of pain and heel function. However, studies describing calcaneal pain and functional status in relation to the length and size of the calcaneal spur are limited and inconclusive [1].According to the literature, about 10% of the population experience pain in the heel, at the site of attachment of the plantar fascia to the tubercle of the calcaneal process, and is usually caused by plantar fasciitis. It is known that plantar fasciitis is associated with the formation of the presence of a calcaneal spur; however, this remains controversial and there is no clear evidence for a link between the two [2].In most cases, various methods of surgical interventions are used to remove a calcaneal spur. With open methods of treatment, osteotomy and excision of the heel tubercle are used. To date, this is an invasive treatment for calcaneal osteophyte [3,4].However, open access is more traumatic. Performing access along the plantar surface of the foot is also traumatic, involving a large number of soft tissues for this operation, long healing, pain and limitation of movement when walking.Also, a method is used to remove the calcaneal spur by accessing the spur, its destruction and subsequent removal, which at the beginning determine the anatomical location of the calcaneal spur using an electron-optical converter, then make an incision along the plantar surface of the foot, bring the trocar to the apical part of the calcaneal spur, from the trocar the tip is removed, the plug is screwed in, due to the impact on which the trocar is placed on the spur, then the plug is removed, a cutter is inserted into the trocar and the spur is cut to the base using a drill [6]. Despite the fact that the method is minimally invasive, access on the plantar surface of the foot is traumatic - a large number of involved soft tissues, long healing, pain and limitation of movement when walking.There is also a known method of endoscopic treatment of painful heel syndromes, including only endoscopic release of the plantar fascia without eliminating other pathological changes, drilling of the calcaneal bone with a bur-shaver, and removal of the calcaneal spur using a modified cannula trocar system [7].
2. Research Objective
- To improve the results of surgical treatment of calcaneal spurs by using endoscopic methods, allowing early activation and rehabilitation of patients.
3. Methodology
- 38 patients aged 26 to 60 years old, 20 men and 18 women, suffering from calcaneal spurs, were studied at RSNPMCTO. All patients underwent surgical treatment in the period from March of 2018 to May of 2021.During clinical examination, all patients had severe pain in the heel area, aggravated by walking, especially the first steps after rest. When examining the heel, edema, local hyperthermia of the skin, and pronounced pain in the heel area were observed on palpation. All patients underwent X-ray, MRI and podometric examination. Based on these data, endoscopic removal of the calcaneal osteophyte was performed.
4. Operation Technique
- Surgical treatment was carried out as follows:The patient, in the supine position, under spinal anesthesia, was on the dorsal surface, in the heel area where the osteophyte is determined, about 1 cm distal to the plantar fascia attachment site, two mini skin incisions were made: lateral and medial, 0.5 cm in size. Through these portals, the endoscope was inserted into the area of the calcaneal osteophyte. The area of the calcaneal osteophyte was gradually filled with 0.9% saline, while shaving was performed under endoscopic observation (pic. 1) changes in the periosteal structure of the calcaneal region were diagnosed (pic. 2).
 | Picture 1. Operational access to the heel region. (outside view Сalcaneal ostophyte) |
 | Picture 2. Diagnosis of changes in the soft and bone tissue of the heel region |
 | Picture 3. Shaving of inflamed soft tissue |
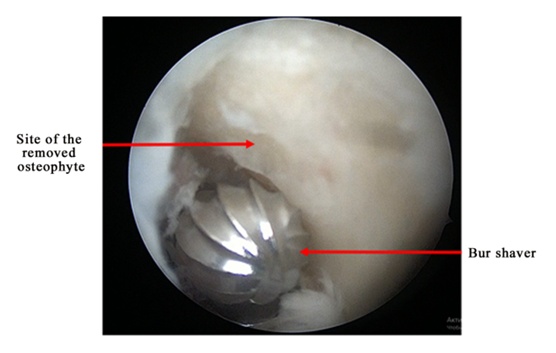 | Picture 4. Bur shaving at the site of bone osteophyte |
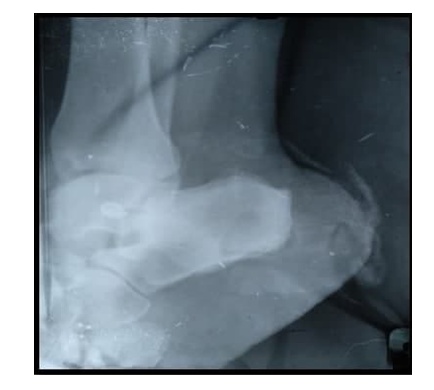 | Picture 5. X-ray image of the heel area after surgery |
5. Results and Discussion
- We studied the results at 3 and 6 months in all patients. Long-term results were studied in 27 patients. Good results were noted in 36 (94.7%) patients, satisfactory in 2 (5.3%) patients. In the postoperative period, immobilization was maintained until the sutures were removed, the load was resolved after 3 weeks. after surgery, depending on the size of the calcaneal osteophyte defect.The method of surgical treatment of calcaneal osteophyte by introducing an endoscope into the region of the calcaneal osteophyte, partial plantar fasciotomy, drilling with a bur shaver and removing the calcaneal osteophyte, consists in the fact that the endoscope is passed through two mini-medial and lateral portals, approximately 1 cm distal to the site of attachment of the plantar fascia - along the dorsal surface of the calcaneus, after fasciotomy, the inflamed soft tissues are shavered and the osteophyte is removed with a shaver with a nozzle, the site of the removed osteophyte is coagulated with an ablator.On the control image intensifier tube, the complete removal of the calcaneal osteophyte is confirmed, in the projection of the removed osteophyte, after suturing, ice is placed on the heel region.The results of studies in our center have shown that endoscopic removal with a shaver with a burr nozzle through two mini skin incisions: lateral and medial, 0.5 cm in size, about 1 cm distal to the site of attachment of the plantar fascia, can reduce trauma to the heel region.The immediate and long-term results of the use of minimally invasive diagnostics and surgical treatment of calcaneal osteophyte in 38 patients were analyzed. All patients received positive results. Analysis of the results showed that technically correctly performed minimally invasive (endoscopic) removal of the heel spur allows to restore normal anatomical relationships and functions in the heel area while maintaining a positive result throughout the observation period.
6. Conclusions
- 1. The proposed method of surgical treatment of calcaneal osteophyte does not have a risk of damage to the main vessels and nerves, since only terminal blood vessels and terminal branches of nerves are present in the surgical area, even their damage will not affect the functional result.2. Shaving of inflamed tissues and removal of the spur with a burr shaver, and coagulation of the site of the removed osteophyte reduces local hemorrhage. Thus, it prevents the formation of rough adhesions and scars in the heel area. Its minimally invasiveness significantly reduces the duration of the operation without negatively affecting the heel area, reduces pain, reduces rehabilitation time and improves postoperative results. Just on the next day after the operation, patients can lean on the operated leg while walking.3. The method of endoscopic treatment of calcaneal osteophyte is convenient and simple, allowing the treatment of patients with calcaneal spurs in a minimally invasive and highly effective way. The developed method can be widely used in practical medicine.