Farmanova M. A., Kasimov I. A.
Bukhara State Medical Institute Named after Abu Ali ibn Sino, Tashkent Pediatric Medical Institute, Uzbekistan
Correspondence to: Farmanova M. A., Bukhara State Medical Institute Named after Abu Ali ibn Sino, Tashkent Pediatric Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
We observed 85 patients aged 17 to 74 years. All patients used standard general, serological, biochemical and statistical methods. According to clinical forms patients were distributed as follows: primary chronic brucellosis (PChB) - 22 (25.8%) and secondary chronic brucellosis (SChB) - 63 (74.2%). The subcompensation phase was observed in 62.3% of the examined patients, the decompensation phase was detected in 37.7%.
Keywords:
Chronic brucellosis, Clinic, Diagnosis, Antioxidant system
Cite this paper: Farmanova M. A., Kasimov I. A., Mechanisms of Peroxide Oxidation in Patients with Chronic Brucellosis and Principles of Treatment, American Journal of Medicine and Medical Sciences, Vol. 12 No. 8, 2022, pp. 815-820. doi: 10.5923/j.ajmms.20221208.10.
1. Introduction
According to WHO data, brucellosis cases are 500 million every year. According to M. Avijgan and co-authors, the number of people infected with brucellosis is 10-25 times more than those registered [2]. According to academician G.G. Onishchenko, the highest prevalence of brucellosis among 100,000 inhabitants was observed in Nepal, the United Arab Emirates, Jordan, Egypt, and Turkey [3]. The epidemiological case of brucellosis in the territory of Russia is not stable, and the incidence is 0.2-0.7 per 100 thousand of the population [4]. The incidence of brucellosis in Kyrgyzstan [7], Georgia, Azerbaijan [3], Kazakhstan [13], Uzbekistan [3], Tajikistan [11] and Turkmenistan from the Commonwealth countries is in high figures and is among 25 high-incidence countries [4]. In Uzbekistan, the incidence rate of brucellosis is 1.8 to 2.8 per 100,000 population [5,8]. In chronic active brucellosis (ChAB), patients complain of periodic body temperature rise, tremors, sweating, malaise, rapid fatigue, muscle, joints, spine pain, headaches, morning stiffness, cold stiffness of hands and feet, dyspeptic symptoms, slowing cognitive function [10]. Clinical, laboratory and functional studies indicate changes in organs and tissues and the presence of multiple focal lesions (fibrosis), as well as lymphatic node lesions. Polyorgan insufficiency, which arises as a result of the systemic effect of brucellas on macroorganism, can lead to a deterioration in the prognosis of the disease. In ChAB, damage to various systems is observed as a result of damage to most organs and tissues [1,6].Various infectious factors faollashtir free radical processes in the body. Polyorgan deficiency, which develops in ChAB, is associated with hemodynamic disorders from multiple disorders, intensification of lipid perecisyl oxidation (LPO). This requires an improvement in the treatment regimen [9,12].Objective: to improve treatment modalities in patients with SFB and to evaluate the effectiveness of phosphargin succinate preparation.
2. Research Materials and Methods
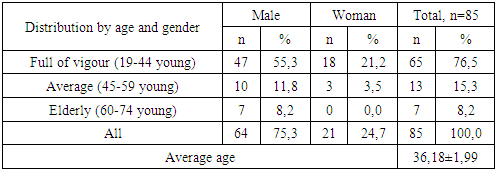
As an object of the study, 85 patients, aged 17-74 years old, who were treated in the Bukhara regional intensive care unit, were taken to the regional endemic centers. Of these, 64 (75,3%) are male and 21 (24,7%) are female. The distribution of patients by age according to WHO classification showed that the incidence was mainly determined by the age of full of vigour (78,5%) (see Table 1). The average age of the patients was 36,18±1,99 years.Table 1. Distribution of patients by age according to WHO classification
 |
| |
|
In the diagnosis of patients, a clinical classification of G.P. Rudnev and N.I. Ragoza, supplemented by K.D. Jalilov, was used. Each patient who came to the hospital was diagnosed according to the results of clinical-epidemiological Anamnesis and laboratory examinations, having passed a clinical examination, an object examination. Hemagglutination reactions and passive hemagglutination reactions were used in the patients. In private investigations, the amount of malondialdehyde in serum was determined by A.I. In Andreeva's method [1], catalase activity was determined by M.Yu. The cortical method [9] and the general antioxidant status were determined by the spectrophotometric method [6], and the C-reactive protein was determined by the enzyme-linked immunosorbent assay. All obtained figures were statistically processed.
3. Results Obtained and Their Analysis
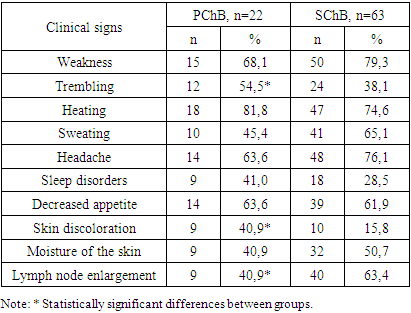
By clinical forms, patients were distributed as follows: primary chronic brucellosis (PChB) - 22 (25.8%) and secondary chronic brucellosis (SChB) - 63 (74.2%). No differences between the sexes in these two forms were identified. In PChB, it was mainly in young people, while in ISB, 73% were young and 20.6% were middle-aged.In all PChB groups, the disease duration was up to 1 year, while in the majority of SChB patients the disease duration was 2–3 years (54.1%), up to 1 year (19.5%), and 4–5 years (1.2%). A subcompensation phase of the disease was observed in 53 (62.3%) patients, and a decompensation phase in 32 (37.7%) patients.Patients mainly complained of fever, weakness, headache, decreased appetite, chills, sweating, and similar manifestations. However, their incidence was different in primary and secondary chronic brucellosis (see Table 2). In particular, if patients with PChB were characterized by weakness, chills, sweating, fever, headache, sleep disturbances, decreased appetite, pale skin, and hydration, SChB often experienced weakness, fever, sweating, headache, and swollen lymph nodes.Table 2
 |
| |
|
It should be noted that locomotor system injuries were more SChB -specific, with the most injuries observed in the knee joint (see Figure 1a), whereas more injuries to the palmar-leg joints were detected in the PChB. At the same time, gastrointestinal lesions were detected in the patients, mainly decreased appetite, tongue covering, and hepatomegaly (see Figure 1b). Gastrointestinal injury was more commonly observed in PChB.Motor system injuries were more SChB -specific, with the most injuries observed in the knee joint (see Figure 1a), whereas more injuries to the palmar-thigh joints were detected in the BSB. At the same time, gastrointestinal lesions were detected in the patients, mainly decreased appetite, tongue covering, and hepatomegaly (see Figure 1b). Gastrointestinal injury was more commonly observed in BSB.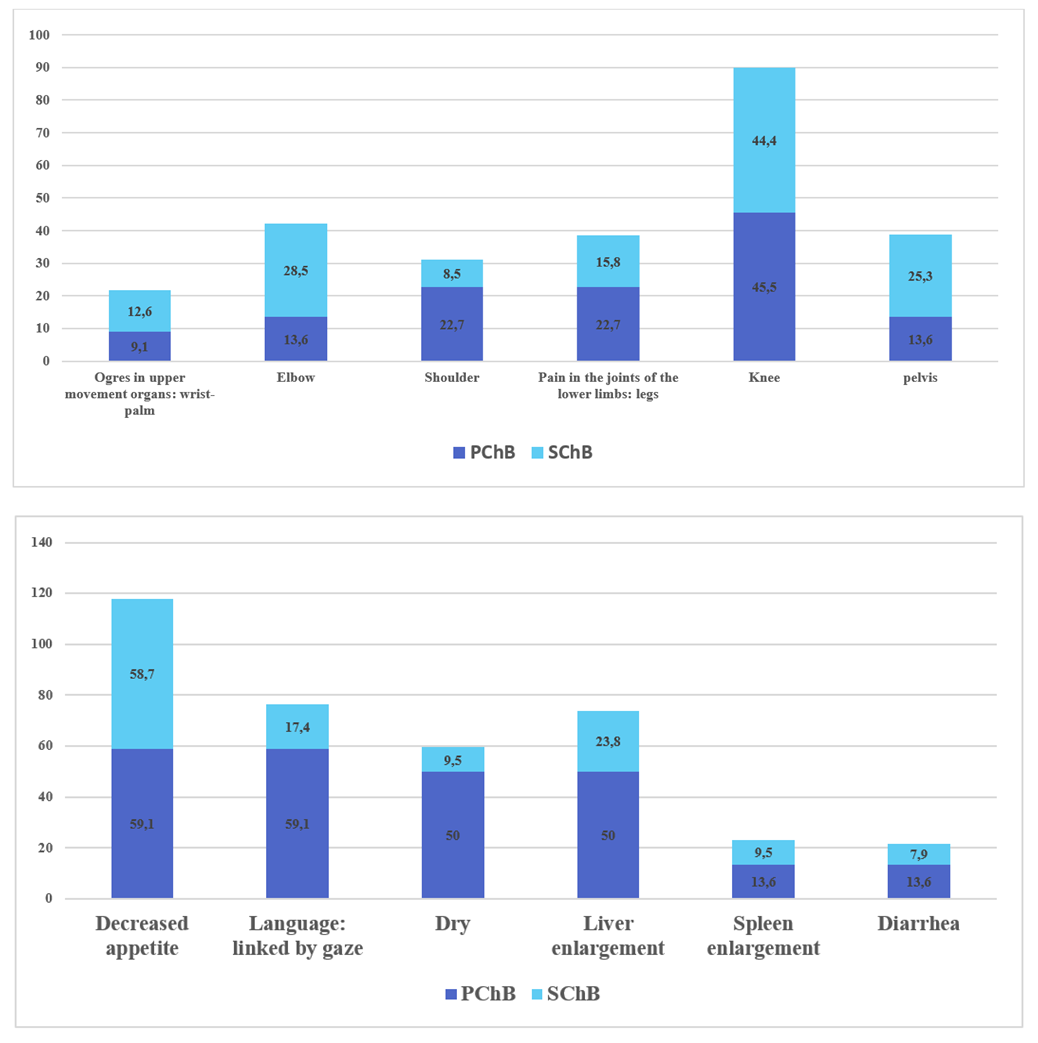 | Figure 1. Diseases of the locomotor (a) and digestive (b) systems according to the form of chronic brucellosis |
Injuries to the cardiovascular system and respiratory organs were mainly observed in primary and secondary brucellosis, characterized by suffocating and hard breathing of the heart tones (see Figure 2a). Nervous system damage neuritis, sleep disorders. In severe forms of brucellosis, genital injuries have also been reported.A subcompensation phase was observed in 62.3% of the patients in the study, and a decompensation phase was detected in 37.7%. The decompensation phase was mainly BSB-specific (see Figure 2b).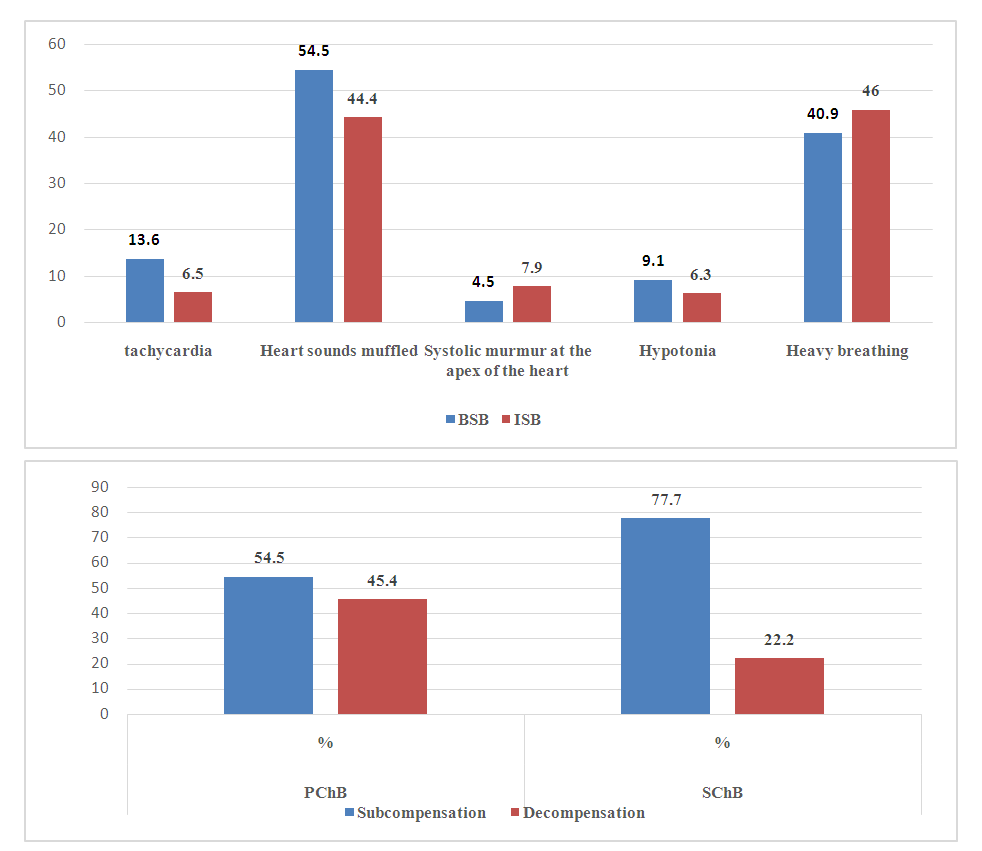 | Figure 2. Diseases of the cardiovascular and respiratory systems according to the form of chronic brucellosis (a) and severity (b) |
Leukopenia, neutropenia, lymphocytosis, and increased ESR were found in the peripheral blood of most patients. Heddleson's reaction was positive in 94.7% of patients, Wright's reaction showed high titers. The titer of the reaction was higher than the titer of RAR, giving a positive result in all patients in the PGAR reaction.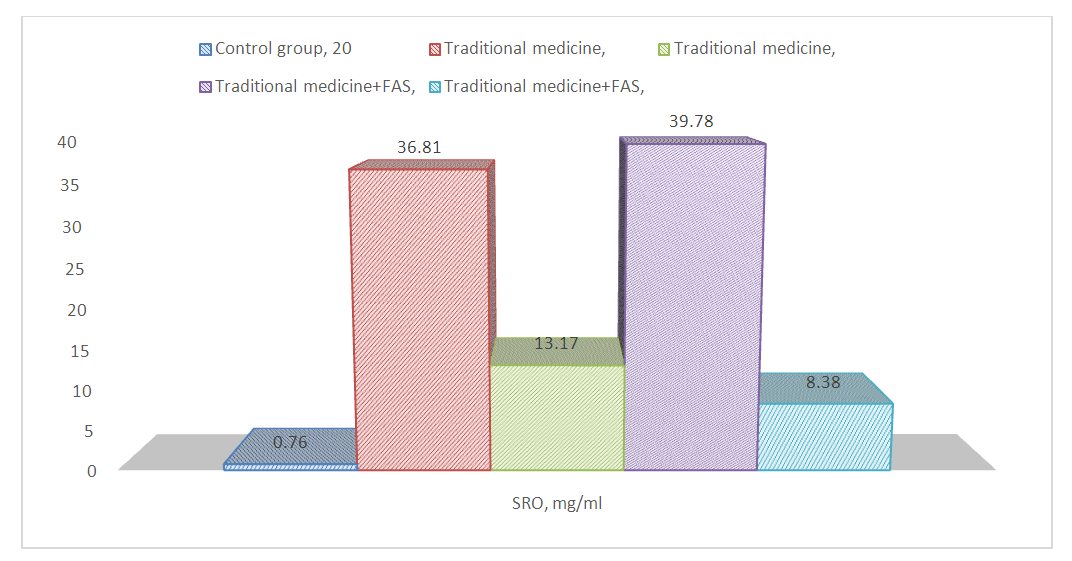 | Figure 3. Changes in serum SRO (mg / ml) according to the form and course of chronic brucellosis |
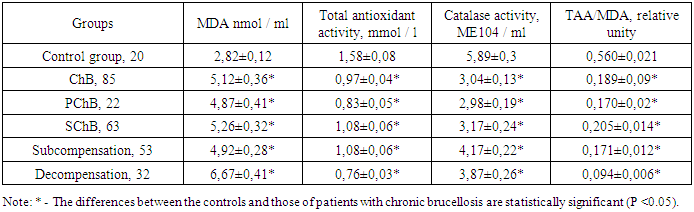
In order to determine the intensity of inflammatory processes, we determined the amount of SRO in the serum of patients. Studies have shown that its amount increased dramatically from 0.76 ± 0.04 mg / mL to 38.14 ± 2.37 mg / mL (P <0.001). Its levels increased to 36.12 ± 2.41 and 39.78 ± 2.19 mg / ml in the BSB and ISB groups, respectively.We also evaluated LPO processes in patients ’serum with MDA levels. The study found a 1.82-fold increase (MD <0.001) in MDA in patients with brucellosis (see Table 3). If in BSB this figure increased 1.73 times (P <0.001), in ISB its increase increased 1.87 (P <0.001). It should be noted that in the subcompensation phase of the disease, the amount of MDA increased by 1.74 (P <0.001) compared to the norm, while in the decompensation phase there was an increase of 2.37 (P <0.001). This indicates that free radical processes are accelerating according to the stages of the disease.Table 3. Changes in LPO and antioxidant system activity according to the form of chronic brucellosis, M ± m
 |
| |
|
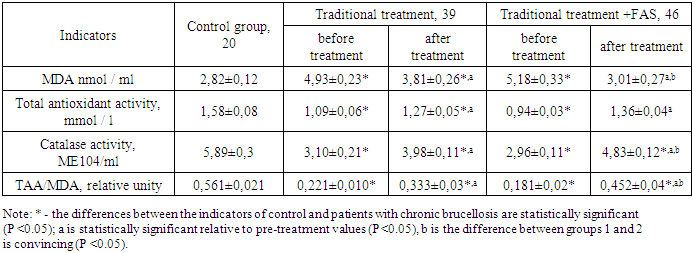
In general, the antioxidant protection system plays an important role in ensuring the normal balance of free oxidation. At present, the assessment of serum antioxidant system reveals general antioxidant activity and catalase enzyme activity. Detection of total antioxidant activity in the serum of patients with chronic brucellosis showed a decrease in this indicator (see Table 3). In particular, in BSB this indicator decreased by 1.9 (P <0.001), while in ISB - by 1.46 (P <0.01). During the subcompensation period of the disease, the total antioxidant activity of the serum decreased by 1.46 (P <0.01) times, while during the decompensation period it decreased by 2.08 (P <0.001). Detection of serum catalase activity showed a decrease in this indicator in patients. In particular, catalase activity decreased 1.98 (P <0.001) and 1.85 (P <0.001) in BSB and ISB group patients. In the subcompensation and decompensation stages, a decrease in enzyme activity was observed by 1.41 (P <0.05) and 1.51 (P <0.01) times.Hence, in SB, an acceleration of LPO, a decrease in total antioxidant protection, and a decrease in serum catalase activity are observed, indicating that such changes indicate a weakening of the compensatory mechanism of the antioxidant chemistry system.Based on the results obtained, we tried to improve the treatment of SB and for this purpose we used the drug phosphargin succinate, which is produced in our country. This drug has antihypoxant and antioxidant properties. Studies have shown that it is more effective than conventional treatment used in the treatment of SB. In particular, conventional therapies reduced serum MDA levels by a statistically significant 1.29 (P <0.05). However, this figure remained 1.35 (P <0.05) times higher in the normative indicators. Although serum TAA and catalase activity increased 1.16 (P <0.05) and 1.28 (P <0.05), the control group reported 1.45 (P <0.05) and 1.9 (P <). 0.01) times lower. This activated the compensatory mechanism of the antioxidant system by 1.5 (P <0.05), but remained 1.68 (P <0.01) lower than the control group.The proposed treatment procedures in the treatment of ChB reduced serum MDA by 1.7 (P <0.01) times (see Table 4). Although this was 1.26 (P <0.05) lower than the group of patients receiving conventional treatment, there was a tendency to be higher than that of the control group. Serum TAA increased 1.44 (P <0.05) times after treatment in group 2 patients. This indicator did not differ statistically convincingly from the indicators of the 1st and control groups. Catalase activity increased 1.63 (P <0.01) times after the proposed treatment. While this was 1.21 (P <0.05) higher than the 1st group, it remained 1.22 (P <0.05) lower than the control group. Such changes have led to an increase in the compensatory mechanisms of serum. Indeed, this figure increased 2.49 (P <0.001) times after the proposed treatment, 1.36 (P <0.05) times higher than the 1st group, but 1.24 (P <0.05) higher than the normative values. ) was kept low. This means that conventional and especially the proposed treatment procedures in the treatment of SB increase the activity of the antioxidant system and weaken the LPO processes.Table 4. Effect of phosphargin succinate on the activity of LPO and antioxidant system in the treatment of chronic brucellosis, M ± m
 |
| |
|
It should be noted that treatment of ChB significantly reduced the amount of SRO statistically. In particular, in group 1 patients, its dose decreased by 2.79 (P <0.001) after treatment, but remained 17.3 (P <0.001) higher than in the control group, indicating the presence of inflammatory processes in the body of patients. In group 2 patients, it decreased 4.75 times (P <0.001). This figure was 1.57 (P <0.01) lower than that of the 1st group, but remained 11.02 (P <0.001) higher than the norm. This indicates that the foci of inflammation have persisted.Hence, treatment of ChB brucellosis reduces the amount of acute phase proteins in the serum, but does not lead to complete normalization. This indicates that the foci of inflammation persist. The proposed treatment reduced the amount of SRO in the serum more effectively than conventional treatment.Of course, the above-mentioned positive results also affected the course of the disease, the complaints of patients decreased, there was a certain regression of changes in various systems. Including if the fever completely disappeared after conventional treatment, weakness, chills, and sweating 1.81; Decreased by 15.36 and 6.03 times, after the proposed treatment - symptoms such as fever, chills and sweating completely disappeared, and fatigue was found to decrease by 5.05 times. Headache, sleep disturbances, skin paleness, and skin moisture 4.0 after conventional treatment; 5.02; Decreased by 3.03 and 9.5 times, insomnia was completely eliminated after the proposed treatment, stomach pain was found to be 17.2 times, skin paleness and moisture were reduced by 30 and 11.11 times, respectively. Lymph node enlargement was reduced from 46.1% to 5.1% in conventional treatment, but from 67.3% to 4.3% after the proposed treatment. This demonstrates the effectiveness of the proposed treatments.Polyorgan deficiency, which develops in chronic brucellosis, leads in large part to hemodynamic disturbances, the acceleration of LPO. This requires improved treatment procedures. In order to restore these processes, the use of the drug Phosphargin succinate produced in Uzbekistan increases the capacity of the antioxidant system compared to conventional treatment and reduces the peroxide oxidation of fats, leading to improved quality of life of patients. This drug is also economically effective. The introduction of phosphargin into the treatment of chronic brucellosis leads to early elimination of clinical signs.
4. Conclusions
1) Chronic brucellosis is accompanied by an increase in the amount of MDA, a decrease in the antioxidant defense system, and a decrease in the compensatory capacity of the antioxidant system, the change of which depends on the severity of the disease.2) In chronic brucellosis, the amount of acute inflammatory protein increases sharply.3) The inclusion of phosphargin succinate in the treatment of chronic brucellosis increases the capacity of the antioxidant system compared to conventional treatment and reduces the peroxidation of fats.4) The introduction of phosphargin in the treatment of chronic brucellosis leads to early elimination of clinical signs.
References
| [1] | Andreeva L.I., Kozhemyakin L.A., Kishkun A.A. Modification of the method for determining lipid peroxides in the test with thiobarbituric acid // Lab. a business. - 1988. - No. 1. - P.41-43. |
| [2] | Avijgan M., Rostamnezhad M., Jahanbani-Ardakani H.. Clinical and serological approach to patients with brucellosis: A common diagnostic dilemma and a worldwide perspective // Microbial Pathogenesis. - 2019. - Vol. 129.- P. 125-130. |
| [3] | Brucellosis. The current state of the problem / ed. G.G. Onishchenko, A.N. Kulichenko. - Stavropol: Gubernia LLC, 2019. - 336 p. |
| [4] | Belozerov E.S. Brucellosis / E.S. Belozerov. - L.: Medicine, 1985. -184 p. |
| [5] | Valiev A.A., Kasymov I.A., Azimov Sh.R. The prevalence of brucellosis infection in children in the Republic of Uzbekistan. - Pediatrics. Tashkent.- 2010. - №1-2.- P.5-8. |
| [6] | Ivanova M.R., Plieva Zh.G. Clinical characteristics and dynamics of some indicators of the antioxidant system (AOS) in patients with chronic brucellosis// Collection of abstracts of the VII Russian congress of infectious disease specialists "New technologies in the diagnosis and treatment of infectious diseases" N.Novgorod. 2006. S. 86. |
| [7] | Kasymbekov J., Imanseitov J., Ballif J. and antibiotic susceptibility of livestock Brucella melitensis isolates from Naryn Oblast, Kyrgyzstan // PLoS Negl. Trop. Dis.- 2013.- Vol.7.– P.2047. |
| [8] | Kasymov O.Sh. Microbiological and genetic analysis of pathogens isolated in brucellosis foci in Uzbekistan and improvement of epidemiological monitoring of the disease // Autoref. diss...tf.d., Tashkent, 2017. - 59 p. |
| [9] | Koralyuk M.A., Ivanova L.I., Mayorova I.G. Determination of catalase activity // Lab. the case – 1988. – No. 1. - S. 16-19. |
| [10] | Lyapina E.P. Chronic brucellosis: systemic inflammation and endotoxicosis, improvement of therapy and epidemiological surveillance: dis. DSc / E.P. Lyapin. - Moscow, 2008. - 310 p. |
| [11] | Rasulov S.A., Mirzoev D.M., Davlatov Kh.O., Akhmatbekova S.Sh. Dynamics of the incidence of brucellosis in small cattle and people in areas of the Republic of Tajikistan with high infection rates // Russian Veterinary Journal. - 2016. - No. 1. - P 22. |
| [12] | Sarkisyan N.S., Ponomarenko D.G., Logvinenko O.V., Rakitina E.L., Kostyuchenko M.V., Kulichenko A.N. Intensity of specific sensitization and immune status in patients with brucellosis. // Medical Immunology.- 2016.- V.18, No. 4. - P. 365-372. |
| [13] | Shevtsov A., Syzdykov M., Kuznetsov A, et al. Antimicrobial susceptibility of Brucella melitensis in Kazakhstan. // Antimicrob Resist Infect Control. - 2017.- Vol.6.- P.130. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML