-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(8): 792-796
doi:10.5923/j.ajmms.20221208.04
Received: Jul. 21, 2022; Accepted: Aug. 5, 2022; Published: Aug. 15, 2022

The Role of Temporary Osteosynthesis in the Treatment of Combined and Multiple Injuries of the Lower Leg Bones
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLI. Y. Khodjanov1, L. A. Amonov2, F. M. Makhsudov2, Yu. R. Malikov2
1Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics, Uzbekistan
2Navoi Branch of the Republican Research Center of Emergency Medicine, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Aim of the research was to study the results of temporary fixation of the shin bones in the treatment of open combined and multiple injuries. Introduction. The number of combined and multiple injuries has continued to increase for the recent years. Mortality rates, according to various authors, range from 16.7% to 49.8% among all injuries of the musculoskeletal system. Fractures of the shin bones occupy the first place among fractures of long tubular bones and, according to statistics, they make up from 20 to 37.3%, open fractures of the shin bones account for 64.3-77.8% of all open limb injuries. Material and methods. A retrospective treatment analysis of 32 patients (27 (84.3%) males and 5 (15.7%) females) treated at the Navoi branch of the Republican Research Center of Emergency Medicine from 2010 to 2022 was carried out. All patients underwent urgent surgical interventions: 5 (15.6%) patients underwent temporary fixation of bone fragments with cross-spokes with a plaster cast, 4 (12.5%) patients underwent temporary osteosynthesis with a bundle of spokes, 21 (65.6%) patients had been applied Ilizarov 's apparatus, a rod external fixation device was applied in 3 (6.3%) cases. Blocking osteosynthesis was performed in 4 patients by a closed method and 7 (21.8%) patients were performed osteosynthesis with LSP plates. Results. The viability of temporary fixation was studied during the period when patients were in osteosynthesis, where the reposition quality of the system and the stability of fragments were determined. Bone fusion was observed in all 32 patients: with dimelic fractures, the fusion period was 84.4 days, with trimelic fractures - 92.7 days. Conclusion. The use of a temporary fixation with the subsequent transition of permanent osteosynthesis in fractures of the shin bones with combined and multiple injuries leads to the fastest withdrawal of patients from a serious condition, to a decrease in the likelihood of infectious complications, early mobilization of the patient and leads to an adequate period of bone fusion.
Keywords: Temporary fixation, Shin bones fracture, Osteosynthesis, Ilizarov's apparatus
Cite this paper: I. Y. Khodjanov, L. A. Amonov, F. M. Makhsudov, Yu. R. Malikov, The Role of Temporary Osteosynthesis in the Treatment of Combined and Multiple Injuries of the Lower Leg Bones, American Journal of Medicine and Medical Sciences, Vol. 12 No. 8, 2022, pp. 792-796. doi: 10.5923/j.ajmms.20221208.04.
1. Introduction
- The number of combined and multiple injuries has continued to increase for the recent years. Mortality and disability rates remain high. Mortality rates, according to various authors, range from 16.7% to 49.8% among all injuries of the musculoskeletal system [1-4]. Multiple fractures of tubular bones occupy one of the leading places in the structure of traumatism and these conditions require urgent trauma care. At the same time, open fractures are verified in 10-18% of cases of the limbs long bones fractures [5-7]. Fractures of the lower leg bones as common are often accompanied by polytrauma. Fractures of the shin bones occupy the first place among fractures of long tubular bones and, according to statistics, they make up from 20 to 37.3% [8], open fractures of the shin bones account for 64.3-77.8% of all open limb injuries [9]. Treatment of shin bones fractures still remains difficult and time-consuming in the structure of traumatic disease [10-11]. Preventive osteosynthesis of limb bones is indicated with the aim of anti-shock measures and stopping blood loss. This is always done with improvised means or external fixation devices (rod or wire devices). Shin bones fractures are most common among fractures of large limb segments in polytrauma [12-13]. Due to anatomical and physiological features, they occupy a leading place in the number of complications - delayed consolidation, non–fusion, deformations, defects, contractures, chronic osteomyelitis [14-15], especially at open injuries. As A.A. Devyatov rightly noted, "... the problem of treating fractures of long tubular bones is, first of all, the problem of treating shin bones fractures " [16]. Currently, most clinics use the tactics of "damage control" in the first and second periods of traumatic disease to improve outcomes. At the same time, surgical treatment of injuries is divided into two stages: upon admission, life-saving surgeries are performed for internal organs injuries, craniocerebral and spinal injuries with temporary stabilization of fractures of large segments of the limbs and pelvis by external fixation devices, and after 5-7 days and later – their final osteosynthesis [17-18]. Aim of the research was to study the results of temporary fixation of the shin bones in the treatment of open combined and multiple injuries.
2. Material and Methods
- We conducted a retrospective treatment analysis of 32 patients (27 (84.3%) males and 5 (15.7%) females) who underwent temporary osteosynthesis (temporary fixation) of the shin bones in order to fix bone fragments during the primary surgical treatment of limb wounds in the Navoi branch of the Republican Research Center of Emergency Medicine from 2010 to 2022. Diagnostic criteria performed: complaints and anamnesis (when the patient is conscious); Laboratory tests: Complete blood count, general urinalysis, biochemical blood test: blood lipid composition; Instrumental research: X-ray of the skull, cervical spine; x-ray of the chest, ECG, ultrasound of the abdominal cavity and pleural cavities; X-ray of the thoracic spine and pelvis; X-ray of various segments of the musculoskeletal system (in different projections according to the location of damage); Computed tomography was performed depending on of the damage location.Combined injuries were detected in 23 (71.8%) patients, multiple injuries - in 9 (28.2%) cases. Due to the occurrence, damages were distributed as follows: accident - in 22 patients (68.7%), occupational injury - in 3 (9.5%) cases, catatrauma - in 5 (15.6%) cases, household injury - in 2 (6.2%) patients (Fig. 1).
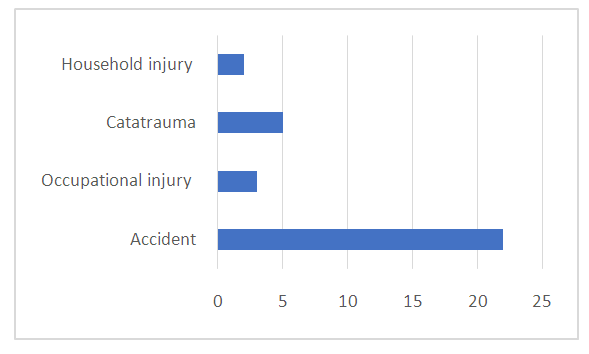 | Figure 1. The cause of injuries |
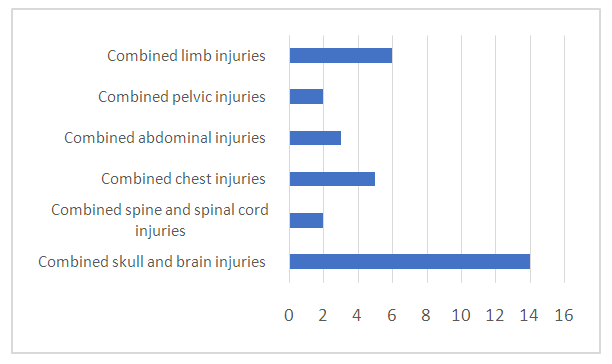 | Figure 2. Distribution of patients by the nature of the leading injury |
3. Results
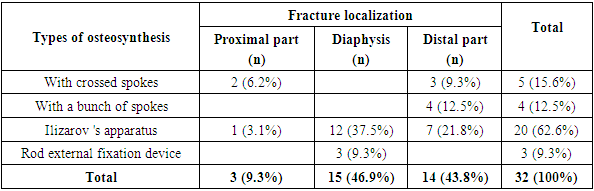
- All patients were admitted urgently and were performed emergency surgical interventions. The duration of the surgery was 20-30 minutes, taking into account the volume of bleeding and the severe condition of the patients. When performing osteosynthesis, it is important to observe the principles of segmentation, the presence of local and regional wounds, the localization and degree of displacement of bone fragments. Taking into account the mentioned above, 5 (15.6%) patients underwent temporary fixation of bone fragments with crossed spoke with a plaster cast, 4 (12.5%) patients underwent temporary osteosynthesis with a bundle of spokes, 21 (65.6%) patients had been applied Ilizarov apparatus, a rod external fixation device was applied in 3 (6.3%) cases.5 patients with the shin bones fractures were performed a temporary osteosynthesis surgery using crossed spokes: 2 patients had a fracture of the proximal tibia, 3 had a fracture of the distal tibia. Three of these patients had an oblique fracture of the tibia with a fracture angle of 45 degrees or more, so two to four spokes were fixed. Two patients had a case of a fragmental oblique fracture of the tibia, while the fracture angle was 45-70 degrees. Up to four crossed spokes were used to fix bone fragments, and the rest of the fragments remained untouched.Four patients had a multi-communited fracture of the shin bones distal part. In these patients temporary osteosynthesis was performed with transarticular bundle spokes through the calcaneus, with a set of 2 to 8 spokes taking into account the diameter of the canal.One patient with a fracture of the proximal part of the shin bones was performed temporary osteosynthesis with Ilizarov 's apparatus with three rings: the first ring was above the knee joint, the second ring was from the proximal part of the tibia, the third ring was located in the diaphyseal part of the tibia. In 12 patients with fractures of the shin bones diaphysis, fixation was carried out by the Ilizarov 's apparatus which consisted of 2 rings.Ilizarov 's apparatus with two rings and a half-ring was installed in 7 patients with fractures of the distal part of the shin bones. The proximal ring was placed through the diaphysis, the second ring was placed through the distal tibia, and the last semiring was installed through the calcaneus.A single-plane external fixation device was used in 3 patients with fractures of the diaphysis of the shin bones (Tab. 1).
|
|
4. Discussion
- Temporary fixation of fractures as one of the main factors in providing anti-shock measures is important when patients admit with polytrauma. Bone fragments are fixed with bundles of spokes, crossed spokes, Ilizarov's apparatus from different layouts and rod external fixation devices at different levels of emergency assistance to victims. The fate of the patient depends on the well-coordinated and skillful work of doctors in providing this assistance. There are many ways to fix preventive osteosynthesis in emergency traumatology. We have used 4 types of fixation from this arsenal in this article. Fixation of bone fragments with crossed spokes is one of the most frequently used methods of temporary osteosynthesis. The method of average stability of bone fragments was used by us in closed and open fractures. The fixation of fragments with good strength qualities of osteosynthesis is achieved by creating an intersection from 60°-90° of the angle between the intersected spokes. The method is easy to use, but requires careful selection of the surfaces of the intersecting spokes. In 5 patients, the method was used with long Ilizarov's spokes with a diameter of 2.2 mm, up to 10 pieces. As far as possible, the spokes were carried through closed sections of the segment, and we tried to create a cross in the bone marrow canal for more stable osteosynthesis.The method of fixation with bundles of spokes, one of the desperate methods of osteosynthesis, is also easy to use due to weakly stabilizing qualities, only for temporary fixation ("until morning"). With dense filling of the bone marrow canal, the method can be left for a long time, that is, until a good recovery of the state of the macroorganism, using two or more (up to 6 pieces) spokes as the length of the fracture line lasts. We used this method in 4 patients with medium-sized closed fractures of the shin bones with the installation of an additional plaster cast. The spokes were removed from 3 to 9 days after the general condition of the body improved, and the patients were transferred to other types of permanent osteosynthesis. Ilizarov’s apparatuses were used in 12 patients for temporary fixation in lightweight versions of the layout consisting of two rings, with the creation of temporary distraction osteosynthesis, they were also fixed in the variants of “shin-femur” and “shin-foot” fractures. A lot has been described about the quality of assistance provided by the Ilizarov's apparatus for preventive osteosynthesis, and we also followed these described methods and achieved the temporary desired effect. After improving the general condition, three patients were used other methods of permanent osteosynthesis, and the in the rest of the patients the device had been rewired with strengthening and adding nodes for permanent stable osteosynthesis.Temporary external fixation devices are increasingly used in the modern world. Methods of hybrid osteosynthesis, arcade systems, methods of single- and multi-plane osteosynthesis are steadily used a lot in the treatment of fractures at polytrauma [19]. We used external rod fixation devices for temporary fixation of bone fragments: in three cases with closed and in two cases with open fractures of the shin bones with good stabilizing qualities. The transition was carried out by installing additional rods with the creation of an arcade version in two cases and hybrid osteosynthesis in one case. This method allowed to quickly restore the basic parameters of life support for patients and allowed other necessary manipulations to be carried out by other specialists. The rods fix bone fragments quite stably and rigidly, have good repositional capabilities for the subsequent easy transition to permanent osteosynthesis without additional fixation. We used this method in three patients with good stabilization of bone fragments and after improving the general condition, two were left in the same fixation after additional installation of two rods directly near the fracture site. One patient was performed a different type of osteosynthesis.
5. Conclusions
- The use of a temporary fixation with the subsequent transition of permanent osteosynthesis in fractures of the shin bones with combined and multiple injuries leads to the fastest withdrawal of patients from a serious condition, to a decrease in the likelihood of infectious complications, early mobilization of the patient and leads to an adequate period of bone fusion.The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.