-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(7): 715-718
doi:10.5923/j.ajmms.20221207.06
Received: Jun. 16, 2022; Accepted: Jul. 8, 2022; Published: Jul. 11, 2022

Clinical and Laboratory Features of Undifferentiated Connective Tissue Dysplasia in the Uzbek Population in Samarkand and Jizzakh Regions
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShodikulova Gulandom Zikriyaevna, Mirzaev Ozod Vohidovich, Atoev Tulkin Tolmasovich
Department of Internal Medicine №3, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Undifferentiated connective tissue dysplasia (UCTD) - is pathology, which united into different syndromes and phenotypes characterized by a variety of clinical manifestations: from benign subclinical forms to multi-organ and multi-system pathology with a progenerative course. The aim of the study presented in this article is to evaluate the clinical and laboratory parameters of patients with undifferentiated connective tissue dysplasia in the Uzbek population using Samarkand and Jizzakh regions as an example. During the last decade the investigators drew attention to the importance of magnesium ions (Mg+2) and metalloproteinases (MMPs) in the regulation of extracellular matrix fibrillar proteins, therefore we used these parameters for the analysis and comparison with the clinical signs of undifferentiated connective tissue dysplasia. Here we present the data proving the correlation between the dynamics of changes in the expression of MMP-2, MMP-9, tissue matrix metalloproteinase-1 inhibitors, Mg+2 ion's concentration and clinical signs in patients with undifferentiated connective tissue dysplasia, which, in its turn, can serve as a method for the evaluation of the pathological process progression and disease prognosis.
Keywords: Undifferentiated connective tissue dysplasia, Uzbek population, Magnesium ions (mg+2), Matrix metalloproteinases
Cite this paper: Shodikulova Gulandom Zikriyaevna, Mirzaev Ozod Vohidovich, Atoev Tulkin Tolmasovich, Clinical and Laboratory Features of Undifferentiated Connective Tissue Dysplasia in the Uzbek Population in Samarkand and Jizzakh Regions, American Journal of Medicine and Medical Sciences, Vol. 12 No. 7, 2022, pp. 715-718. doi: 10.5923/j.ajmms.20221207.06.
1. Introduction
- Undifferentiated connective tissue dysplasia is one of the common connective tissue anomalies. An equally important aspect is the social nature of the problem, as undifferentiated connective tissue dysplasia is often diagnosed in young people, i.e. in the conscript and child-bearing population of Uzbekistan [3,5,8]. These patients are often at increased risk of complications such as severe scoliosis, bone fractures, joint dislocations, infectious endocarditis, thromboembolism, arrhythmias and heart failure. There are no recommendations for the management of such patients in Uzbekistan, particularly with regard to the involvement of the heart and joints in the pathological process, which leads to significant differences in the therapeutic and diagnostic tactics of doctors of various specialities [2,6,9]. The pathogenesis and progression of the disease remain incompletely understood. Among the causes of the formation of undifferentiated connective tissue dysplasia, genetically heterogeneous abnormalities of collagen formation are considered [1,4,10]. An important feature of this process disorder is structural rearrangement of connective tissue elements, extracellular matrix of collagenous fibers and elastin from amorphous substance of glucosaminoglycans and glucuronidases. In the last decade, researchers drew the attention of to the importance of the regulation of fibrillary proteins of the extracellular matrix, magnesium ions (Mg+2) and metalloproteinases (MMPs).Decreased Mg+2- magnesium levels result in endothelial damage, disruption of the spatial organization of collagen and elastin, responsible for the formation of extracellular matrix components, as well as enzymes involved in the process of fibrillogenesis. Low Mg+2 concentrations affect cardiovascular and musculoskeletal system activity, especially the incidence of myxomatous degeneration of mitral valve prolapsing fangs, cardiac arrhythmias. At the same time, disruption of MMP activity leads to damage of the extracellular matrix as a component of stroma that not only serves as a support for cells, but also plays a dynamic role in metabolic processes affecting cell proliferation, differentiation, migration, apoptosis and angiogenesis as well as deposits biologically active growth factors [2,6]. MMPs is now identified as key effectors of tissue remodelling. For a number of reasons, these proteins are expressed in all tissues, at all stages of ontogenesis; they are secreted into the intercellular space and function under physiological conditions; their expression is regulated and activated only under conditions of intense tissue remodelling. Multifunctional MMP proteins are involved in the mechanism of apoptosis and angiogenesis. In addition, they are known to be the only proteolytic enzymes capable of denaturing fibrillar collagens [5,10]. Natural antagonists of MMPs are tissue inhibitors of matrix metalloproteinases and a subfamily of extracellular matrix proteins that regulate and model MMP activity. Nowadays, more than 20 MMPs and tissue inhibitors of matrix metalloproteinases is isolated. The balance between the expression of MMPs and tissue inhibitors of matrix metalloproteinases is unstable both during physiological processes involving tissue growth and development and in various pathologies including undifferentiated connective tissue dysplasias. MMP-2 and MMP-9 are the most common members of the MMP family. These enzymes are able to degrade denatured collagens, fibronectin, laminin, entactin, elastin, etc. It was shown that due to their ability to hydrolyze fibrillar collagen type 4, MMP-2 and MMP-9 stimulate invasive processes related to angiogenesis. The relatively low molecular weight and solubility in biological fluids provide MMP and tissue matrix metalloproteinase inhibitors with the ability to enter the serum in amounts proportional to tissue expression. Therefore, changes in the levels of MMP and tissue inhibitors of matrix metalloproteinases are considered as possible promising biological markers of differential diagnosis, prognosis and treatment of connective tissue dysplasia [2,7,8,10].In view of the above, the aim of the present study was to assess the clinical and laboratory parameters of patients with undifferentiated connective tissue dysplasia in the Uzbek population using the Samarkand and Jizzakh regions as an example.
2. Material and Methods
- The population study included 208 people, including 97 (46.4%) men and 111 (53.6%) women aged 15 to 28 (20.13 ± 0.66) years with undifferentiated connective tissue dysplasia. Depending on the clinical signs and progressive complications the patients were divided into 2 groups, the 1st group of 97 patients with the signs of external phenotypes (phenotypes) of undifferentiated connective tissue dysplasia and the 2nd group of 111 patients with the signs of external and internal phenotypes and some complications. The control group consisted of 20 conditionally healthy persons of comparable age 19.9 ± 1.56 years, without signs of undifferentiated connective tissue dysplasia, who gave voluntary verbal consent for the examination.Blood was taken from the elbow vein in the morning on an empty stomach for serum extraction and determination of: Mg+2 ions in mol/L (AF 610 -A atomic absorption spectrofluorimeter, LTD China); total glycosaminoglycans level in µL/l, glucuronidase activity in µL/l by spectrofluorimetric method (F-96 spectrofluorimeter, LTD China) according to modified method of P. N. Sharayev et al., Activity of matrix metalloproteinases MMP-2 and MMP-9 and tissue inhibitors of matrix metalloproteinases-1. The markers were determined using standard kits for direct ELISA: “Human Mouse/Rat MMP-2 (total)”, Human MMP-9 (total) (Quantikine, “R&D” Sistems) and tissue inhibitor of MMP (“Human TIMP-1, (Biosource)) in accordance with the manufacturer’s instructions. The measurements were performed on an ELISA automatic universal reader (AT-858 LTD China). The concentrations of the test parameters in serum were expressed in ng/ml.
3. Results and Discussions
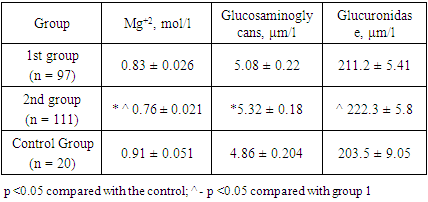
- As can be seen from the material presented, the distribution of men and women was roughly the same, with only a slight predominance of women. Analysis of the SCTD distribution by place of residence showed some predominance of urban residents (121 patients lived in the city, 87 in the countryside). At the same time, we identified features of SCTD morbidity in men and women depending on place of residence. Thus, among urban dwellers the incidence was higher in women (35.7%), and in rural areas it was higher in men (28.5%). As mentioned earlier, UCTD in the studies was mostly characteristic of young people. As can be seen from the above material, patients did not differ significantly by age. A study of sex characteristics showed a predominance of girls (60.8%), but these differences were statistically insignificant. The resulting differences may be due to ethnic and regional characteristics, as patients of Uzbek nationality predominated in our study. Distribution of patients by place of residence showed approximately the same distribution, living in both urban and rural areas. Body weight and BMI were not significantly different in the studied groups of patients, and they were mainly of normal build, in 11.3% and 10.9% of cases there was a hypotrophy, in 6.2% and 7.3% of patients there was some excess of body weight. According to the literature, UCTD is characterized by an asthenic constitution, while we did not find a pronounced asthenic constitution, as normal constitution and malnutrition predominated in 10-11% of cases. In some cases, overweight was also observed. In UCTD, the main external manifestations were hypermobility of the joints of the upper and lower extremities; various changes in the vertebral column as scoliosis or kyphosis; chest deformity; oral pathology manifested by a high palate, abnormal tooth growth and overdentition; flat feet and hallux-valgus, sandal cleft; pronounced skin distensibility and vascular (venous) network in the skin and tendency to form haematomas; eye pathology in the form of astigmatism and myopia; protruding ears with overgrown earlobes; asthenic constitution, etc. The incidence of spinal deformity was studied in 43.6% of patients. Grade 1 and 2 scoliosis was detected in 20.0% and 8.2% of patients, grade 1 and 2 kyphoscoliosis in 7.3% and 2.7% of examined patients, and hyperlordosis in 5.5% of patients. Analysis of the incidence of thoracic deformities in the patients showed their presence in 51.5% of those examined.Cutaneous manifestations of UCTD in the form of varying degrees of skin distensibility were observed in 38.1% and 38.7% of patients. Joint manifestations of UCTD were flatfoot and joint hypermobility. Frequency analysis of flat feet showed their presence in 20.6% and 19.8% of patients. Frequency of combinations of various phenotypes in patients varied, combination of 6 external phenotypes was found in 4.5%, 5 in 10%, 4 in 20%, 3 in 24.3%, 2 in 30.6% of examined patients, and 1 in 11 (10%) patients.The next part of our study involved the evaluation of laboratory parameters in patients with UCTD in the Uzbek population of Samarkand and Jizzak regions.The study showed an increase in MMP-2 and MMP-9 and a decrease in tissue inhibitors of matrix metalloproteinases-1 in the blood of patients with undifferentiated connective tissue dysplasia. As the disease progresses, the expression of MMP-2 and MMP-9 increases and tissue inhibitors of matrix metalloproteinases-1 decreases compared to controls (Table 1).
|
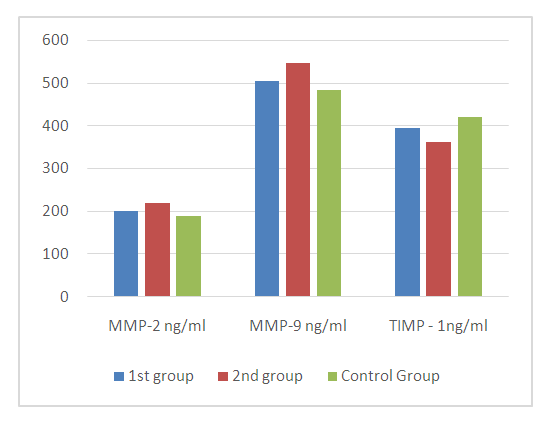 | Figure 1. MMP activity and tissue matrix metalloproteinase inhibitors - 1 in the blood serum of patients with undifferentiated connective tissue dysplasia, M ± m |
4. Conclusions
- In patients with undifferentiated connective tissue dysplasia we revealed the increase of MMP-2 and MMP-9 expression and decrease of tissue inhibitors of matrix metalloproteinases-1 as well as their interrelation with reduction of Mg+2 ions content, induction of glucosaminoglycans and glucuronidases. This was more pronounced in group 2 patients than in group 1. The dynamics of changes in the expression of inhibitors MMP-2, MMP-9 and tissue matrix metalloproteinase-1 depending on the clinical signs in patients with undifferentiated connective tissue dysplasia can serve as a method of evaluation of the pathological process progression and disease prognosis.Conflict of Interest: the authors do not present a conflict of interest.Financial Support: the authors do not hope for financial support.