Mirrakhimova Maktuba Khabibullaevna1, Ikromova Shaxnoza Nazimovna2
1Department of Children's Diseases of the Tashkent Medical Academy, Tashkent, Uzbekistan
2Doctoral Student PhD of the Tashkent Medical Academy, Uzbbekistan
Correspondence to: Mirrakhimova Maktuba Khabibullaevna, Department of Children's Diseases of the Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Connective tissue dysplasia (CTD) is a disorder of connective tissue development in the embryo and postpartum period and is a genetically determined condition characterized by defects in fibrous structures and connective tissue underlying substance. The aimof the study was to study the specific transition characteristics of AG against the background of connective tissue diplasia in children living in Surkhandarya region. The study of the detection of CTD stigmas and dysembryogenesis is particularly important at this stage due to the deterioration of the environmental situation and the change in the classical clinic of the disease.
Keywords:
Glomerulonephritis, Dysplasia, Connective tissue, Children, Stigmas of dysembryogenesis
Cite this paper: Mirrakhimova Maktuba Khabibullaevna, Ikromova Shaxnoza Nazimovna, The Role of Connective Tissue Dysplasia in Children with Acute Glomerulonephritis, American Journal of Medicine and Medical Sciences, Vol. 12 No. 7, 2022, pp. 703-705. doi: 10.5923/j.ajmms.20221207.02.
1. Introduction
Connective tissue dysplasia syndrome (CTDS) is a genetically heterogeneous condition that, according to the literature, is highly detectable in children with renal pathology, including pyelonephritis, interstitial nephritis, cystitis, nephroptosis, glomerulonephritis [3]. Dysplastic changes in connective tissue significantly affect homeostasis, metabolism and immunity and are manifested by the progressive course of various morphological and functional disorders in tissues, organs and the body and determine the characteristics of the associated pathology [6,7].Connective tissue performs many functions: morphogenetic, biomechanical, trophic, barrier, structural, etc., the leader of which is the integration of different organs and tissues of the body as a whole [1]. Morphological changes in connective tissue, changes in metabolic processes, immunogenesis, lead to the appearance of secondary disorders in the internal organs, which often determine the severity of the underlying pathological process [2,4]. Unfavorable environmental factors leading to the formation of "secondary environmental immunodeficiency" affect the metabolism of connective tissue, the state of cell membranes, so the negative effects of CTD are more pronounced in such patients [5,7].CTDS is characterized not only by external signs, but also by a decrease in T-lymphocyte activity, CD3 +, CD4 + deficiency, phagocytosis, changes in IgA, IgM, IgG levels, formation and elimination of circulating immune complexes (CIC), decreased activity and intensity of macrophage-monocyte immunity appears in [4]. This leads to the development of immunopathological and immunocomplex diseases, including acute glomerulonephritis (AG), which has a specific clinical course.
2. Materials and Methods
We examined 94 children aged 1 to 15 years living in Surkhandarya region with OGN, who were being treated at the Regional Children's Clinical Hospital and City Children's Hospital №1 AG was present in 58 patients with nephritic syndrome, in 22 patients with nephrotic syndrome (NS), and in 14 patients the disease was observed with NS and hematuria. All patients underwent conventional clinical and laboratory examination, which included the detection of CTD stigmas and dysembryogenesis. The degree of disorganization of the main substance of the connective tissue was determined by the level of cialic acids, seromucoids, C-reactive protein, CIC, cryoglobulins.
3. Results and Discussion
Examination of 94 children with AG revealed CTD stigmas in 84.04 ± 3.78% of patients, multiple CTD stigmas (3 or more) in 39.36 ± 5.04%, i.e., this condition was observed in every third patient with AG. Anomalies of the arms and legs (41.49 ± 5.08%) and flat feet (40.43 ± 5.06%) were the most common of the CTD stigmas (photo 1).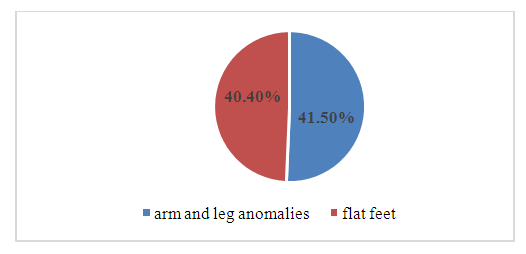 | Photo 1. The most common BTD stigmas |
Pigment spots and hypermobility of the joints were observed at the same frequency (33.98 ± 4.89%) and postural disorders, scoliosis, were detected in 20.21 ± 4.14% of patients. Other CTD stigmas (chest deformity, hernias, myopia, high neck, long fingers, gallbladder deformity, mitral valve prolapse) were observed in 10% of the examined patients. More than 5 CTD stigmas were detected in 3 of 94 children. Absence of CTD stigmas was found in 15.96 ± 3.78% of children with AG. In different forms of AG, CTD stigmas occurred at almost the same frequency (r >0.05). In patients with nephritic syndrome (39.66 ± 6.42%) and nephrotic syndrome (40.91 ± 10.73%), three or more CTD stigmas occurred at equal frequency. These features of metabolism and immunity in children with CTD may indicate a tendency to develop AG, but do not determine its form. Because CTD is genetically determined, specific features of connective tissue metabolism may occur during the fetal period, which affects the formation of some stigmas of dysembryogenesis. 91.49 ± 2.88% of patients with AG had disembriogenesis stigmas, and 51.06 ± 5.16% had multiple disembriogenesis stigmas (3 or more) in children, i.e., observed in every second patient with AG. Of the dysembryogenesis stigmas, the syndactyly tendency of the second and third toes is the most common (78.72 ± 4.22%), with the same frequency - arched palate and hypertelorism (56.38 ± 5.11 and 52.13 ± 5.15, respectively). %), less ear supra deformity (20.21 ± 4.14%), forehead hair growth was observed (18.09 ± 3.97%). Other stigmas of disembryogenesis, such as skull-shaped anomalies, epicanthus, renal anomalies, eye anomalies, cryptorchidism, additional sucking in the chest, hypertrichosis, occur in less than 5% of children examined. More than 5 stigmas of dysembryogenesis were observed in 8 of 94 children (8.51 ± 2.88%).Observations of dysembryogenesis stigmas in different forms of AG have led to a number of differences. In the nephrotic form of AG, there were 3 or more dysembryogenesis stigmas than in the nephritic form, which were detected in 68.18 ± 10.20% of patients with nephrotic form and 41.38 ± 6.47% of patients with nephritic form. (r <0, 05). However, 1-2 stigmas of dysembryogenesis were detected more in only 5 out of 22 patients with nephritic syndrome (28 patients, 48.28 ± 6.56%) and nephrotic syndrome (r <0.05).The presence of multiple dysembryogenesis stigmas in patients with nephrotic syndrome indirectly indicates the negative impact of connective tissue metabolism, membrane permeability, immunity, its regulatory systems (cytokines) on the occurrence of nephrotic syndrome in AG. The frequency of dysembryogenesis stigmas in isolated urinary syndrome did not differ from the frequency in AG with nephritic syndrome, so these two groups of patients were not separated. The nature of the dyembriogenesis stigmas did not differ significantly (r> 0.05) in groups of patients with different forms of AG.The presence of a combination of CTD stigmas and dysembryogenesis was found in almost all patients with AG (98.94 ± 1.06%). CTD stigma and dysembryogenesis were not detected in only one child. It was a school-age boy who fell ill after a sore throat. In this child, AG continued with nephritic syndrome. The majority of children (84.04 ± 3.78%) had more than 3 stigmas of CTD and disembriogenesis, with only 14.9 ± 3.67% of children having AG nephritic syndrome, 1-2 stigmas of CTD and disembriogenesis. No child with nephrotic syndrome had less than 3 stigmas of CTD and dysembryogenesis. However, the majority of all children with nephrotic syndrome and the majority of children with nephrotic syndrome with hematuria (13 out of 14) had more than 3 stigmas of CTD and dysembryogenesis. The combination of more than 5 stigmas of CTD and disembriogenesis was observed in 54.26 ± 5.13% of patients, i.e., observed in every second patient with AG. The presence of 5 or more stigmas of CTD and disembryogenesis was more pronounced in nephrotic syndrome (68.18 ± 10.20%) and in nephrotic + hematuric syndrome (78.57 ± 11.40%) than in nephritic syndrome (43.18 ± 11.40%). significantly more common.Thus, the presence of multiple stigmas of CTD and disembriogenesis in a patient with AG may be an indirect criterion for predicting the severity of the process, damaging not only the glomerular apparatus but also the basement membrane. Because AG with nephrotic syndrome and AG with nephrotic syndrome were more common in patients with multiple stigmas of CTD and dysembryogenesis, the clinical manifestations in these patients had certain characteristics. In patients with AG with CTD stigma, edema syndrome was more common in anasarca (39.20 ± 5.49%) and in patients with moderate edema (16.46 ± 4.17%, r <0.05) and in children with AG without CTD stigma, dominated the eyelids and legs (80.00 ± 10.69%, r <0.01). The tumor persisted longer (12.32 ± 1.05 days) in patients with AG with CTD stigma, and the duration of tumor in patients without CTD stigma was 8.07 ± 1.31 days (r >0.05). Macrohematuria is less common in patients with AG without CTD stigma (86.70 ± 9.08%, r >0.05). Its duration does not depend on the presence or absence of CTD stigmas. Proteinuria up to 1 g / l In patients with AG without CTD stigma (73.33 ± 11.82%), proteinuria up to 2 g / l was observed in patients with AG with CTD stigma (r <0.05). The daily average rate of proteinuria was 2.6 times higher in patients with CTD stigma than in patients without CTD stigma. The degree of leukocyturia does not depend on the number of CTDs (r >0.05).Acute phase parameters (cialic acid, diphenylamine test (DFA), seromucoid, C-reactive protein), CIC and cryoglobulins, fibrinogen levels were significantly increased in patients with AG with CTD stigma. This is because the presence of CTD stigmas reflects some features of the metabolism of connective tissue structures, acute phase parameters, levels of CIC and cryoglobulins were analyzed depending on the presence or absence of fibrinogen CTD stigmas.Thus, in patients with AG with CTD stigma, tsial acids were elevated in 62.75 ± 6.77% of cases, with an average rate of 261.0 ± 11.0 units; DFA increased by 70.59 ± 6.38%, the average level of DFA was 0.290 ± 0.011 units; seromucoid increased in 49.02 ± 7.00% of patients, its mean level was 0.32 ± 0.01 op.pl. n patients with AG without CTD stigma, sialic acid, DFA, and seromucoids were elevated in only 1/6 of patients, and the mean level of sialic acid was 182.5 ± 17.0 arb units, DFA - 0.210 ± 0.017 u.p. (p <0.01), seromucoid - 0.22 ± 0.02 op.pl. (r <0.001). The mean level of C-reactive protein in the presence of CTD stigmas was 4.6 times higher than in patients without CTD stigma (r <0.01). The mean fibrinogen level was slightly higher in the presence of CTD stigmas (4.40 ± 0.36 g / l, r> 0.05). The number of CTD stigmas affected the growth phase of acute phase parameters, CIC, cryoglobulins, fibrinogen. In patients with multiple CTD stigmas, all of these rates were found to be high.
4. Conclusions
1. The majority of children with AG have CTD and disembriogenesis stigmas, one in three children have multiple CTD stigmas, and one in two children have multiple disembriogenesis stigmas. Significantly, 5 or more stigmas of CTD and disembriogenesis are detected in AG with nephrotic syndrome and in AG with nephrotic syndrome with hematuria and hypertension. 2. The presence of multiple stigmas of CTD and dysembryogenesis, on the one hand, indicates a negative effect in the ante- and postnatal period, which is prone to the development of AG. 3. The study of the detection of CTD stigmas and dysembryogenesis is particularly important at this stage due to the deterioration of the environmental situation and the change in the classical clinic of the disease.
References
| [1] | Arsentev V. G., Baranov V. S., Shabalov N.P. Nasledstvennыe zabolevaniya soedinitelnoy tkani kak konstitutsionalnaya prichina poliorgannyx narusheniy u detey. - SPb.: SpetsLit., 2014. |
| [2] | Kadurina, T.I. Dysplasia of connective tissue. Rukovodstvo dlya vrachey / T.I. Kadurina, V.I. Gorbunova. - Spb.: ELBI, 2009; 704-708. |
| [3] | Liss V.L., Skorodok Yu.L., Plotnikova E. V., and dr. Diagnosis and treatment of endocrine zabolevaniy u detey i podrostkov (uchebnoe posobie) / Pod red. N. P. Shabalova. - M.: MEDpress-inform, 2017. |
| [4] | Mambetova A.M., Shabalova N.N., Inarokova A.M., et al. Influence of dysplasia of connective tissue on the treatment, production of hormones and cytokines in children with priobretennymi zabolevaniyami kidneys in vide glomerulonephritis, hemolyticouremicheskogo syndrome and secondary pyelonephritis // Pediatr, 2018; 6– 6. |
| [5] | Mirraximova, MX., Ikramova, ShN. Soedinitelno-tkannye dysplasia in children with chronic glomerulonephritis / European journal of science archives conferences series. -2022. DOI https://doi.org/10.5281/zenodo.5889885. |
| [6] | Poliorgannыe narusheniya pry dysplasiyax soedinitelnoy tkani u detey. Diagnostic algorithms. Tactics of vedeniya. Rossiyskie rekomendatsii // Voprosy detskoy dietologii. 2017; 3: 53–79. |
| [7] | Mirrahimova M.Kh., Agzamkhodzhaeva N.S., Ikromova Sh.N. Influence of connective tissue dysplasia on the course of glomerulonefritis in children /Galaxy International Interdisciplinary Research Journal. 2022; 10(5): 928–931. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML