-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(6): 677-681
doi:10.5923/j.ajmms.20221206.14
Received: May 9, 2022; Accepted: Jun. 1, 2022; Published: Jun. 23, 2022

The State of Protein Metabolism in Chronic Tubulointerstitial Nephritis in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhmatova Yulduz Ablakulova, Akhmedjanova Nargiza Ismailovna, Akhmatov Ablokul, Yuldashev Botir Akhmatovich, Rakhmanov Yusup Abdullayevich
Department of Pediatrics No. 2 of Samarkand State Medical University, Uzbekistan
Correspondence to: Akhmatova Yulduz Ablakulova, Department of Pediatrics No. 2 of Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The achievements in the diagnosis and therapy of neurological diseases in children are enormous, but nevertheless, in about 23% of patients, the disease has a progressive course, which significantly affects the formation of the quality of life. A survey of 120 children with CTIN, aged from 4 to 15 years, was conducted. Considering the clinical variant of CTIN, all patients were divided into 2 groups: group 1 – 52 (43%) children with recurrent form of CTIN and group 2 - 68 (57%) patients with latent CTIN. Among them, there were 65 boys (54%), 55 girls (46%). The conducted studies have shown that with the development of rCTIN and lCTIN, an important mechanism of damage to interstitial kidney tissue, the development of clinical symptoms and the course of the disease is both a metabolic disorder leading to structural shifts at the level of various elements of the nephron and changes in the functional state of the kidneys, and instability of the cytomembranes of tubular cells.
Keywords: Protein metabolism, Chronic tubulointerstitial nephritis, Endogenous intoxication, Instability of cytomembranes
Cite this paper: Akhmatova Yulduz Ablakulova, Akhmedjanova Nargiza Ismailovna, Akhmatov Ablokul, Yuldashev Botir Akhmatovich, Rakhmanov Yusup Abdullayevich, The State of Protein Metabolism in Chronic Tubulointerstitial Nephritis in Children, American Journal of Medicine and Medical Sciences, Vol. 12 No. 6, 2022, pp. 677-681. doi: 10.5923/j.ajmms.20221206.14.
1. Introduction
- The achievements in the diagnosis and therapy of neurological diseases in children are enormous, but nevertheless, in about 23% of patients, the disease has a progressive course, which significantly affects the formation of the quality of life. The inflammatory process in the tubulointerstitial tissue (TIT) of the kidneys progresses against the background of specific and nonspecific etiological factors. Interstitial kidney tissue is a focus of pathology in the TKD that further covers the blood, lymphatic vessels and tubules of the renal stroma [5,7,9].Renal glycosuria is defined as the excretion of glucose in urine in a normoglycemic state. It results from renal tubular dysfunction or immaturity of tubular function in the newborn. Etiologically, renal glycosuria is of 3 types-benign renal glycosuria, glycosuria with diabetes mellitus (including gestational diabetes) and tubular defects (Fanconi syndrome). Prognosis of benign renal glycosuria is excellent and reversible. Acute interstitial nephritis (AIN) is one of the main causes of acute renal failure and may often result in tubular dysfunction. In this study, the authors report the occurrence of AIN with acute renal failure that contributed to reversible renal glycosuria. The glycosuria observed in the patient of this study was an isolated tubular defect, with no phosphaturia, aminoaciduria or bicarbonaturia. Such a presentation is very rare in adults and has not been previously reported. These findings confirm that AIN with acute renal failure can cause an isolated tubular defect with benign reversible glycosuria in an adult [5].Microscopic data of TIN are: infiltration (lymphoid or macrophage) of interstitial tissue with transition to loose - or coarse-fibrous sclerosis, dystrophy and/or atrophy of the tubule epithelium [4,10].Studies of recent decades have proven an important role in the origin of the TKD of molecules of kidney damage. They can participate simultaneously in many processes of endotoxin formation and their accumulation in the internal homeostasis of the body [1,2,6,13]. A number of authors have noted that endotoxicosis is a cascade process [8,9,12].Despite the successes achieved in the treatment and prevention of CTIN in children, there is currently no exact algorithm for the diagnosis of this pathology in the literature. Comparative clinical and laboratory diagnostics of the main types of tubulointerstitial nephritis is also not fully developed. There is no data on the pathogenetic relationship between tubular functions and indicators of protein metabolism of blood serum and urine in children with different forms of CTIN. The development of a new pathogenetically based complex treatment of CTIN in children remains a significant research task.
2. Aim
- To develop a method for the complex correction of CTIN in children, considering the identified pathogenetic significance of the parameters of endogenous intoxication and violations of tubular functions.
3. Materials and Methods
- This study presents the results of examination and treatment of 120 children with CTIN, in the phase of active inflammatory process, who were in the pediatric nephrology department of the children's regional multidisciplinary scientific Center of Samarkand, in the period from 2019-2021.Considering the clinical variant of CTIN, all patients were divided into 2 groups: group 1 – 52 (43%) children with recurrent form of CTIN and group 2 - 68 (57%) patients with latent CTIN. Among them, there were 65 boys (54%), 55 girls (46%). The patients underwent general clinical, laboratory and instrumental examinations.The clinical diagnosis of CTIN was carried out according to the diagnostic criteria proposed in the classification of N.A. Korovina (2003), where special attention was paid to the characteristics of the pedigree anamnesis: the definition of IC, TIN, ICD, metabolic disorders at an early age, which were symptoms of exudative catarrhal diathesis, dysuric disorders against the background of crystalluria."Urinary syndrome" was characterized by: abacterialleukocyturia, high osmotic density of urine, microproteinuria, microhematuria, crystalluria.The control group consisted of 30 practically healthy children who did not suffer from chronic diseases, who had not been ill for the last 6 months, with a favorable nephrological family history at the age of 4 to 15 years.Renal indicators were assessed during the period of exacerbation of the disease, during the formation of clinical and laboratory remission, 1 year, 2 and 3 years after the period of exacerbation. The study did not detect children with CTIN on the background of severe congenital pathology in combination with impaired functional state of the kidneys.The state of renal functions was assessed on the basis of two groups of functional techniques:group I - methods indicating the quantitative state of renal functions of various parts of the nephron.a) The state of renal filtration function (clearance of endogenous creatinine) was assessed according to the Van Slyke formula:Using immunoturbidimetry on the Cobas Integra 400 plus apparatus (Roche, Switzerland), cystatin C was determined:- this is a protein that is formed in the nucleus of cells at a constant rate;- has the property of free filtration in the glomeruli;- inversely correlates with GFR and is highly sensitive to its changes compared to its changes in creatinine [9];- it is metabolized in the proximal tubules during reabsorption;- it is formed regardless of gender, body weight or tumors of the presence of inflammatory processes;To determine the concentration capacity of the kidneys, a Zimnitsky sample was used. In addition, the value of ammonioacidogenesis was determined (titrated acids and ammonia were determined in the daily urine).Protein metabolism parameters (protein fractions, total serum protein, total and effective albumin concentration, serum toxicity index, albumin binding ability) were determined in all examined patients. Serumurea and creatinine levels were also determined.
4. Results and Discussion
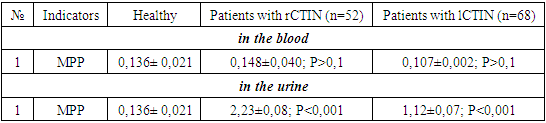
- The clinical group (group 1: 52 patients) with rCTIN was isolated based on the presence of typical signs of the disease, such as dysuria (32.7%), neurogenic bladder (10%), pasty soft tissues of the eyelids in the morning (46.5%), lower back pain (30.8%) on the background of physical activity (26.9%).Whereas, the clinical group (group 2: 68 patients) with lCTIN was isolated on the basis of a more permanent symptom of "losing kidney", which leads to the development of muscular hypotension - 41.2% (28) and arterial hypotension – 27.9% (19), dysuria – polyuria in 54.4% (37) patients, the presence of abacterial lesions of renal tissue against hyperoxaluria – 100% (68), an abundance of epithelium in 92.6% (63), lympho– monocytic character - 88.2% (60), brown cylinders – 100% (68). Urine culture is sterile.Diagnostic criteria for the latent course of CTIN: they were detected against the background of respiratory diseases, they did not receive attention due to their short duration, hereditary history was not considered.In our studies, a high percentage of the incidence of the continuously recurrent form of CTIN occurred in children aged 10-14 years, which accounted for 43.2% of the total number of patients with the continuously recurrent form of CTIN.We associate the recurrent course of the disease with the presence of a secondary immunodeficiency condition, the indirect signs of which are: frequent recurrence (more than 2 times a year) and prolonged course (preservation of clinical and laboratory signs for more than 6 months), short-term effect of antibiotic therapy, multiple foci of chronic infectious pathology, susceptibility to acute respiratory viral infections.In the clinical status of patients with chronic recurrent TIN, the frequency of exacerbation of the disease over the past period was determined and revealed that in 20 (38.7%) children the frequency of exacerbation was 1 time per year, in 19 (36.5%) children 2 times a year and in 12 (23.1%) children more than twice a year.The parameters of protein metabolism were determined in all the examined patients (total serum protein, OKA, ECA, protein fractions, CSA, altered albumin concentration and toxicity index, MPP in urine and blood, globulin fractions, cystatin C concentration, albumin functional status indicators, urea, creatinine levels).Currently, it has been established that with the development of multiple organ and polysystem insufficiency, the products of impaired metabolism – endotoxins - accumulate in the body. Endotoxins include products of natural metabolism that accumulate in the body in high concentrations, MPP - intermediate products of proteolysis, variable products, heterogeneous ingredients of non-viable tissues that accumulate in the body when the natural mechanisms of detoxification and metabolic disorders are suppressed [9]. There is a direct relationship between the degree of EI and the volume of MPP in the urine, depending on the severity of CTIN [6,8].Studies of kidney function and EI indicators are necessary to predict the course of CTIN. The degree of damage to the membrane structures of kidney cells was assessed by the level of MPP and OCA in the urine, in the blood by the total concentration of albumin, ECA, CSA, IT and KIA.The data obtained showed that the concentration of MPP in the urine of patients with rCTIN in the acute phase was 16.3 times higher than the control group (Table 1.), whereas in children with lCTIN it was 8 times higher. There were more pronounced violations of cellular structures in patients with rutin compared with patients with lakhtin.
|
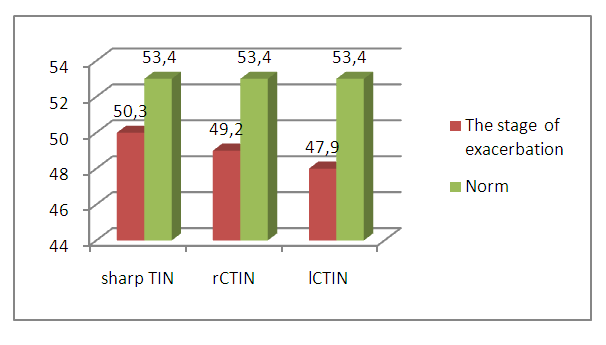 | Figure 1. OCA indicator in the acute stage in various forms of the disease in children |
|
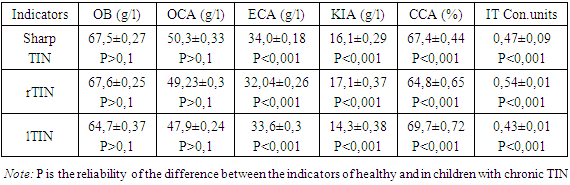
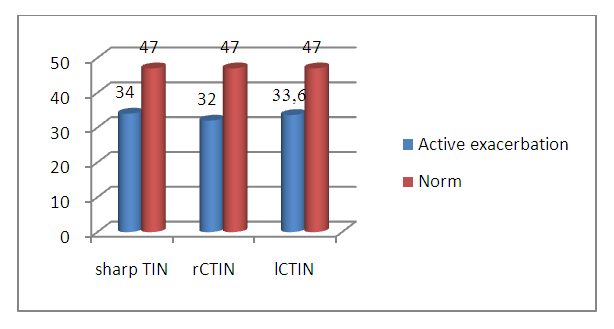 | Figure 2. The indicator of ECA in the active stage in various forms of CTIN in children |
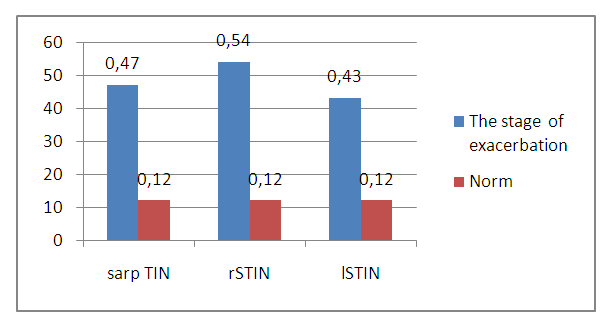 | Figure 3. IT indicator in the active stage in various forms of the disease in children |
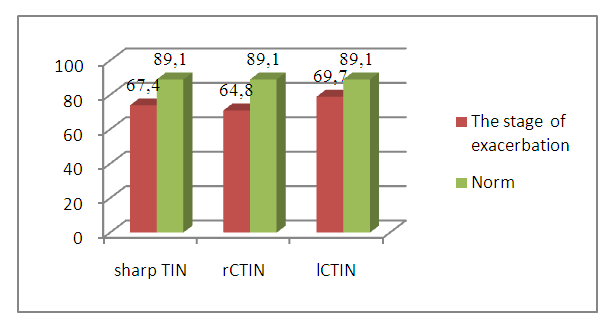 | Figure 4. Indicators of CSA in the active stage in various forms of CTIN in children |
5. Conclusions
- Thus, the conducted studies have shown that with the development of rCTIN and lCTIN, an important mechanism for damage to interstitial kidney tissue, the development of clinical symptoms and the course of the disease is both a metabolic disorder leading to structural shifts at the level of various elements of the nephron and changes in the functional state of the kidneys, and instability of the cytomembranes of tubular cells. This justifies the need for combination therapy in patients with CTIN, which will contribute to the elimination of the inflammatory process, the excretion of endotoxins from the renal tissue, stabilization of cellular cytomembranes and kidney functions.