-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(5): 573-578
doi:10.5923/j.ajmms.20221205.25
Received: April 21, 2022; Accepted: May 16, 2022; Published: May 24, 2022

Clinical and Pathogenetic Features of Neuralgia of Trigeminal Nerve in Patients of the Elderly and Senile Age
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLG. T. Matchanov, Sh. T. Niyozov, A. T. Jurabekova
Samarkand State Medical Institute, Samarkand, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Neuralgia of trigeminal nerve (HTN) is characterized by severe pain attacks, the mechanism of formation of which is described in numerous literary sources, where the authors describe various pathogenetic concepts with the development of treatment methods. This work was no exception, the study was conducted on the basis of a private clinic, the features of clinical and pathogenetic aspects of NTN in elderly and senile patients were studied, observing the stages of diagnosis; laboratory and instrumental indicators were studied, where deformation of the trigeminal nerve openings due to osteoporosis was proved. The cause itself was determined as compression-tunneling; optimization of treatment with a chondroprotective drug revealed high positive results.
Keywords: Neuralgia of trigeminal nerve, Elderly and senile age, Diagnosis, Treatment
Cite this paper: G. T. Matchanov, Sh. T. Niyozov, A. T. Jurabekova, Clinical and Pathogenetic Features of Neuralgia of Trigeminal Nerve in Patients of the Elderly and Senile Age, American Journal of Medicine and Medical Sciences, Vol. 12 No. 5, 2022, pp. 573-578. doi: 10.5923/j.ajmms.20221205.25.
Article Outline
1. Introduction
- Since the time of Hippocrates and Galen, there have been descriptions of signs of neuralgia of trigeminal nerve [1,3,4]. According to WHO data, neuralgia of trigeminal nerve is a fairly common disease and occurs within 5-6 cases per 100 thousand population. The main component of the disease is a painful attack (more often on the one hand). Many literary sources describe the mechanism of occurrence of neuralgia of trigeminal nerve (NTN), in their opinion there are many discrepancies; some consider the cause to be hypothermia, others associate it with an infection that has joined or already exists. Based on the recommendations of the International Association for the Study of Pain (IASP), neuralgia of trigeminal nerve should be presented as a syndrome characterized by pain in the areas of innervation of the branches of the trigeminal nerve, most often on one side of the face, the pain is acute, occurs suddenly, under the influence of a provoking factor (for example, with incorrect or not natural facial movement, with activation of facial muscles) (Manvelov A.S. et al., 2013). According to the National Guidelines for 2010, NTN occurs 1 case per 15 thousand people, with a predominant lesion in people over 50 years old, and over the past 5 years, according to WHO, the prevalence ranges from 30 to 50 cases per 100 thousand population, in 60% of cases it is localized on the right, the incidence of the disease is predominantly female (https;//www.pet-net.ru), the same sources have shown that according to WHO, NTN data, 1 million people suffer worldwide.Balyazin E.V. (2014), having studied in detail the features of a painful attack, connects this syndrome with areas of non-painful stimuli, the mucous membrane of the mouth, teeth, tongue or skin. The duration of the attack is short from a second to several minutes, but has an interval frequency during the day. Very importantly, the author notes that the duration of remissions decreases with age. According to the classification, NTN is described by the following clinical signs as typical, idiopathic, classical, cryptogenic, essential (Grachev Yu.V. et al., 1999, Dambrovsky V.I. et al., 2009, Zinchenko A.P. et al., 1981, Markunae R.S., 1984, Sapon N.A., 2005, Crucen G, 2004, Long E. et al., 2005, Kanoto M. et al., 2012).Modern views on the etiology of NTN remain controversial. So, Livshits L.Ya, (1968) in 70% of patients associates the cause with a high-ranking pyramid of the temporal bone, on the side of the pathological process, the root irritation factor. Rubin L.R. (1966), explains the cause of the pain attack, again by the anatomical defect of the lower bite. Later, Balyazina E.V. (2012) regarded the disease as a secondary process, a consequence of otitis media, and sinusitis with the formation of adhesions in the bridge-cerebellar region. The following scientists (Karlov V.A., 1980, Amador N. et al., 2008, Broggi G., 2004, Erbay S.H. et al., 2006, Laurent B. et al., 2009, Miller S.P., 2009) turned out to be supporters of the theory of neurovascular conflict. The detection of neurovascular conflict has become possible thanks to the MRI (CT) included in medical diagnostics, especially with the use of a three-dimensional image. Kress B.S. et al. (2006) after conducting a study, they found in 73% of cases a neurovascular conflict, where 61% is associated with an artery. The authors, in addition to the conclusions, recommend that patients with NTN undergo MRI neuroimaging to all, without exception, as a standard of diagnosis, to differentiate the disease, symptomatic NTN from other forms, in particular idiopathic (Sandell T. et al., 2010).According to Tsymbalyuk V.I. et al. ((2007), Makhambetov E.T., Shpekov A.S., Berdikhodzhaev M.S., Smagulov F.H. (2011), about nerve compression in the region of the ponto-cerebellar bridge [2,6], and as a result, ischemia of the trigeminal nerve system. The reason is presented somewhat differently by researchers studying the state of the anatomical structure of the bite or age-related bone changes that irritate the nerve and lead to pain syndrome [5,7]. Stepanenko (2019) points out in his works that 6% of disorders are associated with compression of plaques on the background of multiple sclerosis. According to the theory of Melrack R., the portal theory; in which, with a decrease in myelinated fibers, the effect on the nuclei of the spinal trigeminal nerve increases, thereby increasing the pain threshold. There are very few literary sources where the association of NTN with osteoporosis, a condition in which the calcium content in bones decreases, is very insignificant. In the work, Troyan V.V. (2005) uses differentiated treatment of NTN, according to the author, 63% of patients with NTN are women over the age of 65 who have menopause and signs of osteoporosis. By the author Oganesyan G.R. (2016), in order to improve the treatment of trigeminal pain, dental aspects of disorders and myofascial pain were studied in patients older than 70 years (up to 81 years), additional studies were conducted on the bone structure of patients, spondylarthrosis, osteoporosis were determined, the conclusion in the research work was, the mandatory use of orthopantomography in patients with NTN since it is necessary to have a complete picture of the relationship of the bone structure of the maxillofacial zone.A wide range of nonsteroidal and chondroprotective drugs is used to relieve pain and improve the results of degenerative-dystrophic diseases. A randomized study (in Russia) was conducted on 600 patients, using the drug Aflutop, Osteochondritis, Chondroitin glucosamine sulfate divided into groups. Patients were diagnosed with severe pain syndrome, MRI – osteochondrosis, osteoporosis, protrusions, herniated discs with compression of the spine, the average age was from 50 to 70 years. The result of the study showed that Alflutop has a high analgesic effect, contributes a significant positive effect to the degenerative-dystrophic process of the spine and dramatically reduces the risk of chronic pain syndrome (Radoutskaya E.Yu. et al., 2019). Professor M.S. Svetlova (2014) conducted 5-year observations on the use of Aflutop in patients with gonarthrosis, showing the need for long-term treatment, safety of the drug, good tolerability, without side effects, reliability of positive dynamics and improvement of the quality of life of patients. In 2014, Lunina G.V. et al. the tolerability and efficacy of Aflutop were studied in patients with osteoporosis, where there was a significant decrease in intra-articular glialin cartilage, without progression over a year, with very good tolerability. From the data of the review literature analysis by G.P. Khasenova (2017), Aflutop has been used since the 90s in more than 50 countries of the world, studies by authors in countries (Romania, Belarus, Azerbaijan, Kazakhstan, Moldova, Ukraine, etc.) have reliably proven the effectiveness of the drug.Balyazina E.V., Isakhanova T.A., Balyazin V.A., Bondareva O.I., Balyazin-Parfenov I.V., Kadyan N.G. (2017), went further and put forward their hypothesis about the consequences of the autoimmune process, linking the stomatological procedure of intervention, after which the neurology of the trigeminal nerve develops. The authors studied the titer of antibodies to the main protein of myelin, proving the process of demyelination. In addition, the occurrence of NTN in old age is likely to be explained by the vascular factor of the disorder, the atherosclerotic or pathological nature of the shape of the vessels compressing the nerve root [8,9]. Practice shows that there is a need for further research of NTN in the elderly and senile patients, since according to a literature review, more than 65% of the pain syndrome in NTN occurs in people from 60 to 70 years old. The relevance is related to another factor, patients of this age, out of 70%, only 10% are treated with NTN by a neurologist, which indicates ignorance and the need to optimize treatment tactics.
2. Aim of Investigation
- To study the neurology of the trigeminal nerve in the elderly and senile patients, clinical and pathogenetic features, with the development of a modern approach to diagnosis and treatment.
3. Materials and Study Design
- The study was conducted in a private clinic in Samarkand, elderly and senile patients (from 60 to 75 years old), for the period 2020-2022, in the number of 40 people, with neurology trigeminal nerve, were subject to observation. The criteria for inclusion, in addition to age, pain syndrome of the trigeminal nerve exit points, was compliance with the (Boston) algorithm, where identifying trigeminal zones of HTN on one side, there was no sensitive disorders on the other side. The ratio of gender differences was 3:1, there were more women. The exclusion criteria were patients younger than 60 years of age, patients with comorbid background, diabetes mellitus, tumors (in particular, the bridge of the medullary region), post-traumatic changes, the consequences of surgery in the area of the projection of the trigeminal nerve.All patients underwent a standard clinical neurological examination, an MRI examination of the brain, more to clarify the age-related deformation of the skull shape, on the MRT – Signa Exporer device (2020).In several cases, computer angiography of the brain was performed; in some cases, ultrasound transcrianal dopplerography of branchiocephalic vessels has been carried out. Laboratory blood test for the presence of calcium in the blood (Ca), ionized (normally 1.16-1.32 mmol/L), (solid-phase chemoluminescent enzyme immunoassay). Densitometry was performed in order to determine bone density and the presence of osteoporosis (this method was studied in the SAFO TIBBIYOT private clinic) for all patients. The treatment is described in the results of the study. Statistical data were evaluated on an individual computer, with standard Student indicators.
4. Results
- The reason for the treatment of patients was pain in the face area, at a certain point, unilateral pain was characterized by patients as “dagger” or electric shock. The duration of pain on average did not exceed two minutes, with a frequency of every half hour or one hour. The duration of the disease is different for everyone, 3 people suffered in this position for several days, took painkillers, patiently waited for the situation to change for the better by itself. 7 people underwent a long stage of treatment at the dentist, maxillofacial surgeon, with partial temporal dynamics, and turned with an exacerbation of the process. Most of the patients have already turned to neurologists, and the treatment was carried out on an outpatient basis, the remission was, according to the patients, prolonged for almost a year, there were 13 such patients; the rest of the patients used non–traditional methods of medicine to relieve the pain syndrome – acupuncture, application of leeches, lotions, phytotherapy; in these cases, remission lasted from 2 to 4 months.The diagnosis of NTN consists of classical, standard assessments. First of all, characteristic complaints of paroxysmal pain in one half of the face, by the type of electric shock, or burning. Patients change facial expressions close their eyes; grab their face with their hand (from the side of pain). During an attack, the patient does not give the opportunity to examine (fear of pain, makes him sit motionless), and in the period between the attack, when pressing on the points in the middle of the eyebrow arch, in the cheek area (along the line of the tip of the nose), the mandibular point, gives soreness either along all the listed lines, or only at one specific point. Radiation of pain is given to the area of the ear or teeth (one patient removed a tooth, such a strong pain attack spread to the jaw area). The pain in 2 patients spread to the neck area. Important in the diagnosis was the collection of anamnesis, indicating the strength of the pain, a description of the nature, time of the attack, the causes of the provoking pain, the duration of the attack, the timing of the disease, than the patient relieves the pain.During the clinical and neurological examination, there were no focal symptoms (if we do not take into account age-related characteristic changes characteristic of all patients with dyscirculatory encephalopathy, convergence disorder, slight smoothness of the nasolabial fold on one side, slight deviation of the tongue, difference in tendon reflexes, etc.). It turned out to be important, the special behavior of the patient, when trying to check the trigeminal points for pain irritation, the fear of increasing pain, made the patient shy away from this check. The gentle position of the head was characteristic, since any attempt to change the position ended with a painful blow. This condition was detected in 9 patients, and was considered as severe, patients refused to take food, water, because, again, because of the fear of repeated pain, that is, the treatment to the clinic had to be during the period of exacerbation. If we consider the extent of pain during the day, then patients complain of pain throughout the day, but the increase occurs in the evening and at night. The intensity of pain was controlled, according to the visual analog scale (VAS), very strong, corresponded to 10 points in 9 patients; strong, within 9 points in 27 patients; in 6 patients it remained moderate to 7 points. In 70%, localization of pain paroxysms was observed on the right side, in the rest on the left side, which corresponded to the literature data. Foreign authors explain the process of difficult-to-treat treatment in the elderly and senile people with NTN by the fact that there is a double blow, both from the demyelination of peripheral fibers, which degenerate and die with age, and from the central nervous system, where demyelination is a response in the form of perceptual pain, to neurovascular conflict (l).In accordance with the tasks set, additional research methods were carried out to study the pain syndrome in elderly and senile patients with NTN, in addition to the analysis of clinical and neurological examination. According to the assumption, in addition to the above-shown deminizing processes in the central nervous system and peripheral nervous system, there is a fact of tunnel syndrome, due to age-related changes in the skull bone itself, against the background of osteoporosis characteristic of this age group. The first step in this direction was to check laboratory parameters for the quality of ionized calcium (cation), which does not depend on protein in the blood, which allows it to be used as a criterion for calcium metabolism to detect osteoporosis.The analysis for the determination of ionized calcium was carried out in the morning (since, by the evening, the calcium values were higher); it turned out that all the examined patients had low ionized calcium values below one, the average value corresponded to 0.8±0.1 mmol/l; which presupposes prerequisites for osteoporosis in older age. The next stage confirming osteoporosis was a direct examination on the apparatus, dexitometry, to study bone density, the diagnostic method allows to determine the signs of osteoporosis in the early subclinical stages. After 50 years, the fragility of bones increases, due to thinning, turns into a “porous bone”; osteporosis affects the entire skeleton. The causes of osteoporosis are numerous, the basis includes metabolism disorders, it is characteristic of every person, but in some people the process is expressed quite intensively [7,6]. Quantitative ultrasound densitometry (KUDM) was used in the work (previously, patients were warned that they should not take calcium medications per day). Important survey indicators, assessment of T and Z points, T-score (normally 1) the examined patients had an average of 2.3±1.0 points, which serves as a diagnosis of osteoporosis; regarding the Z-score, the figures corresponded to age indicators.According to many scientists, an MRI examination of patients with NTN is an important component for differentiating the diagnosis, pure or classical NTN, from secondary compression, for example, by a tumor. In our cases, the interest of MRI research is connected, in addition to the above, with the study of bone structure, or rather deformity in the elderly and senile, against the background of proven osteoporosis. Computer angiography was performed in the vertical plane, the intersection of the trigeminal nerve root at the level of the lateral part of the pontomesencephalic segment. The method itself had a drawing in 3D format.
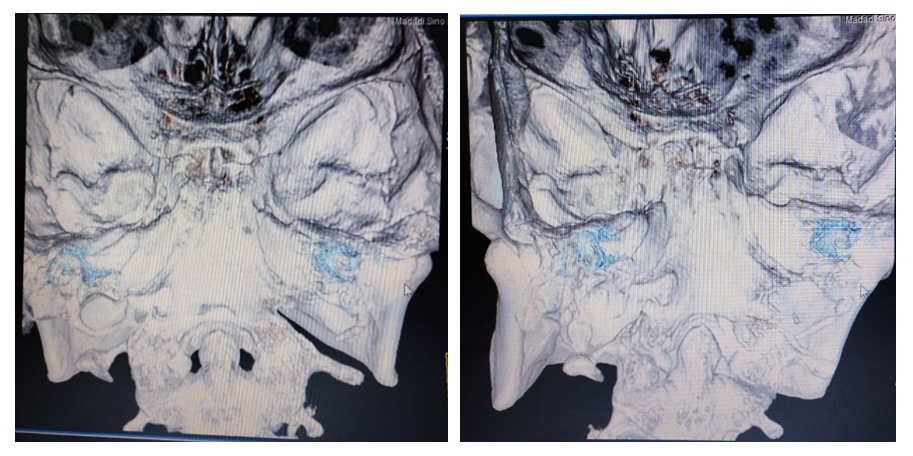 | Figure 1. Patient Z. neuralgia of trigeminal nerve with localization of pain in the zone of the second branch. Round hole on the right 0.9 mm, on the left 1.1 mm |
5. Conclusions
- Thus, our task was to study the features of NTN in elderly and senile patients. The study revealed that in all 40 patients with NTN, the duration of the disease ranges from one year to several years. Remission is short, the right half of the face suffers more often, the most pronounced pain points are in the area of the oval and round holes.Examination of patients for the presence of ionized calcium revealed low figures of 0.8 mmol/L and quantitative ultrasound densitometry revealed an average T-score of 2.3±1.0 points, which serves as a diagnosis of osteoporosis.A 3D computer study of the bone structure of the facial part determined changes, deformity associated with age-related disorders and the level of osteoporosis, the presence of trigeminal nerve openings of different diameters in volume, which creates a compression-tunnel syndrome that causes pain attacks (before treatment 4.5±0.5 mm2, 5.4±0.5 mm2 on the right side, after treatment 5.2±0.5 mm2, 6.3±0.5 mm2, in the area of the round hole and the subglacial, respectively).The proposed therapy with the drug Alflutop revealed positive results, both as an analgesic drug that reduces the use of NSAIDs, and as a drug that creates complete remission (78%) of cases in elderly and senile patients with NTN.
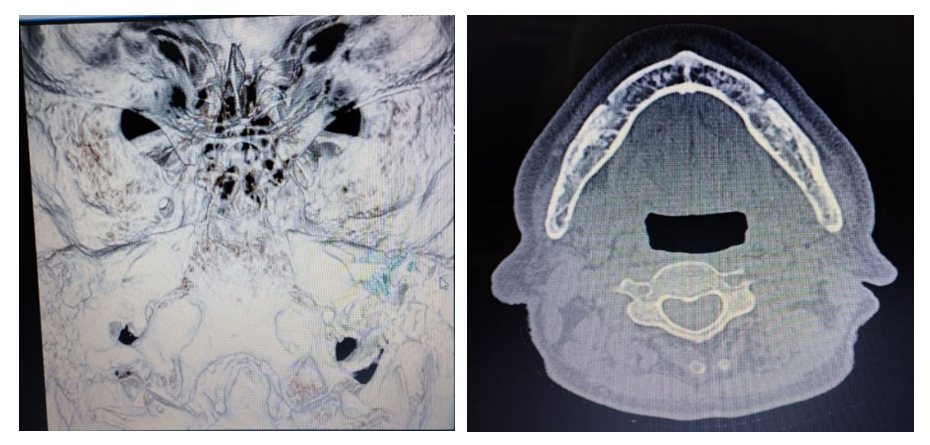 | Figure 2. Patient D. neuralgia of trigeminal nerve with localization of pain in the zone of the second branch. The round hole before the treatment is 0.7 mm on the right, 1.1 mm on the left. After treatment, the round hole on the right is 1.0 mm, on the left 1.4 mm |
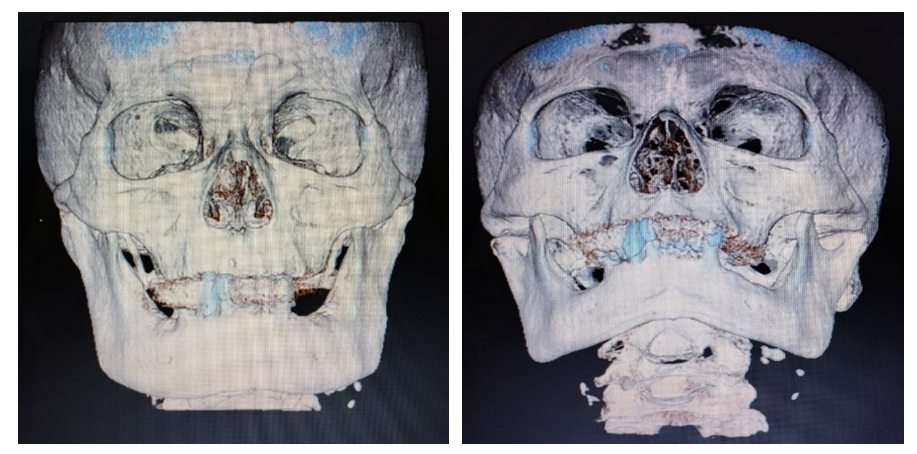 | Figure 3. Patient D. neuralgia of trigeminal nerve with localization of pain in the zone of the second branch. The opening of the upper jaw before treatment is 0.6 mm on the right, 0.5 mm on the left. After treatment, the hole on the right is 1.1 mm, on the left 0.9 mm |