-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(5): 551-553
doi:10.5923/j.ajmms.20221205.19
Received: April 20, 2022; Accepted: May 11, 2022; Published: May 14, 2022

Systemic Inflammatory Response in Patients with Exotoxic Shock with Acute Acetic Acid Poisoning
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKuvatov Zokhid Hayitovich
Bukhara Branch of the Republican Scientific Research Center of Emergency Medicine, Uzbekistan
Correspondence to: Kuvatov Zokhid Hayitovich, Bukhara Branch of the Republican Scientific Research Center of Emergency Medicine, Uzbekistan.
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Due to the wide availability of acetic acid, acute poisoning with acetic acid is one of the most common etiological factors of household poisoning throughout Uzbekistan, and their proportion is quite large from 8.5 to 14.7%, and the mortality rate reaches 19-22.5% [one]. Materials and Methods: The study was conducted in 78 patients with acute acetic acid poisoning. As indicators of inflammation activity, the following were studied: the content of IL-6, IL-10 and procalcitonin (PCT) in blood serum. Results: An increase in the content of IL-6 in the blood of patients to a level of 54-214 pg/ml was determined upon admission. With the development of sepsis, an increased concentration of IL-6 (up to 115 pg/ml) was observed up to the fifth day. The content of IL-10 in the blood of patients with subsequent development of sepsis at admission was significantly higher (56-113 pg/ml) than in the blood of patients without sepsis. The concentration of IL-10 correlated with the development of sepsis (r = 0.8) and the incidence of deaths (r = 0.5). The content of PCT increased from the third day in patients with sepsis to a level exceeding the diagnostic value for sepsis (2 ng/ml).
Keywords: Acetic acid poisoning, Interleukins, Procalciotonin, Systemic inflammatory response, Sepsis
Cite this paper: Kuvatov Zokhid Hayitovich, Systemic Inflammatory Response in Patients with Exotoxic Shock with Acute Acetic Acid Poisoning, American Journal of Medicine and Medical Sciences, Vol. 12 No. 5, 2022, pp. 551-553. doi: 10.5923/j.ajmms.20221205.19.
Article Outline
1. Introduction
- Severe acute poisoning with acetic acid (UA) causes the development of tissue hypoxia associated with disturbances in the acid-base state and the direct inhibitory effect of high doses of drugs on respiratory enzymes [1]. - and hepatotoxic effects due to hemolysis of erythrocytes, the development of toxic coagulopathy, disseminated intravascular coagulation syndrome [5,7]. The cauterizing effect is most pronounced in the respiratory tract and in the gastrointestinal tract. Not only the mucous membrane is necrotic - the process can spread to the entire thickness of the submucosal and muscular layers [4,6]. When taking UC, a burn disease of chemical etiology develops due to a local destructive effect on tissues and its resorptive effect. As a result of massive plasma loss, there is a decrease in the volume of circulating blood, and at the same time a decrease in all indicators that reflect central hemodynamics: cardiac output, stroke and minute volumes of the heart, central venous pressure and blood flow velocity, which forms the development of acute circulatory failure, which is classified as exotoxic shock (ES) of the hypovolemic type [3,6,7]. One of the main characteristic signs of the development of systemic inflammation is an increase in the concentration of inflammatory and anti-inflammatory cytokines in the blood [2].Burns of the upper gastrointestinal tract, intravascular hemolysis and decompensated metabolic acidosis in patients with acute acetic acid poisoning quickly form disorders of transcapillary metabolism, vascular platelet hemostasis, oxidative processes, promote activation of blood coagulation and fibrinolysis, which leads to the development of DIC [4,5]. Exotoxic shock is the cause of death in acetic acid poisoning on the first day [7]. Therefore, the main objectives of the intensive therapy of ES is the early elimination of volemic disorders with simultaneous improvement of microcirculation, respiratory function, relief of metabolic acidosis and hypoxia [7,8].The purpose of the study was to identify early markers of the development of the systemic inflammatory response syndrome and manifestations of sepsis in patients with severe acute acetic acid poisoning.
2. Materials and Methods
- The study was carried out in 78 patients with acute UC poisoning (mean age 31.6 ± 4.3) who were admitted to the intensive care unit of the Bukhara branch of the RNCEM. The comparison group consisted of 35 healthy volunteers (mean age 32.5±5.2). The severity of the patients' condition was due to ES, toxic encephalopathy, which manifested itself as impaired consciousness from stupor to coma II-III degree. The treatment included infusion therapy, relief of pain and ES, which includes the introduction of narcotic drugs (morphine, promedol, omnopon), neuroleptanalgesia, anticholinergics (papaverine, atropine, platifillin) subcutaneously 3-5 times a day, forced diuresis with obligatory blood alkalization ( up to 800-1500 ml of 4% sodium bicarbonate intravenously to relieve hemolysis), the introduction of colloid and crystalloid solutions in a ratio of 1: 3 (in severe cases up to 8-12 l) with the simultaneous administration of 4-12 ml of torsid under the control of CVP, as well as antibacterial and symptomatic therapy. The development of systemic inflammatory response syndrome (SIRS), sepsis was determined by the presence of signs presented in the recommendations of the International Guidelines for Severe Sepsis and Septic Shock (TheThirdInternational Consensus Definitionsfor Sepsisand Septic Shock - Sepsis-3 (2016)). The severity of multiple organ failure associated with sepsis was assessed using the SOFA scale (1994) adopted by the European Society for Intensive Care. The degree of hypoxia in the victims was assessed by the level of PaO2 in the arterial blood. As indicators of the activity of inflammation, the following were studied: the content of IL-6, IL-10 and procalcitonin (PCT) in the blood serum. Studies were performed upon admission of patients to the hospital, 24 hours later, on the 3rd and 5th days after poisoning. Upon admission and on the 3rd day after the incident, the patients underwent bacteriological examination of the material from the mucous membrane of the pharynx, urine and blood in order to identify pathogenic and opportunistic microflora.
3. Research Results and Discussion
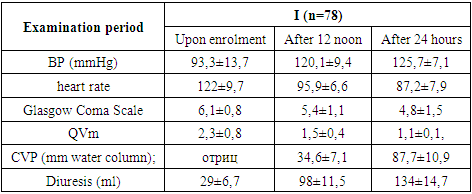
- In acute poisoning with acetic acid, the clinical picture in all patients was characterized by depression of consciousness to the level of coma of I-II degree (6.1 ± 0.8 points on the Glasgow Coma Scale). A coma in case of poisoning with acetic acid was accompanied by the development of acute respiratory failure of mixed genesis. The central mechanisms of respiratory depression were combined with obstructive disorders as a result of bronchorrhea and hypersalivation.
|
4. Conclusions
- 1. In patients with acute exacerbation of acute acid reflux, there is a development of SSVO, caused by hypoxia (rO2 = 68.5 ± 6.5 mm Hg), which occurs in the hospital.2. K 3-5 sutkam posu postupleniya u 14% bolnyx nablyudali razvitie septicheskogo sostoyaniya, laboratornym prediktorom kotorogo v 1 sutki yavilos vыsokoe soderjanie v krovi IL-10 (v 15 raz i bolee).3. Increased content in the blood of IL-6 (more than 115 pkg / ml) and procalcitonin (more than 2 ng / ml) for 3 days after toxic exposure can be considered as early diagnostic criteria for the progression of sepsis.