-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(4): 386-389
doi:10.5923/j.ajmms.20221204.04
Received: Mar. 2, 2022; Accepted: Mar. 23, 2022; Published: Apr. 15, 2022

Structure of Patients with Multiple Myeloma According to the Data of the Republican Specialized Scientific-Practical Medical Center of Hematology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNasibakhon Xodjiakbarovna Kakhkharova1, Abdurakhmon Abdumavlyanovich Kayumov2
1Clinical Department, Republican Specialized Scientific-Practical Medical Center of hematology (RSSPMCH) MoH RUz, Uzbekistan, Tashkent
2Administration, Republican Specialized Scientific-Practical Medical Center of Hematology (RSSPMCH) MoH RUz, Uzbekistan, Tashkent
Correspondence to: Nasibakhon Xodjiakbarovna Kakhkharova, Clinical Department, Republican Specialized Scientific-Practical Medical Center of hematology (RSSPMCH) MoH RUz, Uzbekistan, Tashkent.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to examine the structure and distribution of patients with various forms of multiple myeloma (MM) in Uzbekistan. The study was carried out at the Republican Specialized Scientific-Practical Medical Center of Hematology (RSSPMCH) of the MoH RUz. The highest incidence of patients with MM diagnosis was recorded from Tashkent city (19.7%), Tashkent region (23.0%), Fergana region (17.2%), Kashakadarya region (10.7%). The structure of pathological protein was investigated in the majority of patients. Studies of pathological protein heavy chain in MM revealed A-chain in 15 patients and G-chain in 77 patients, which was 12.3% and 63.1% respectively. This work will allow us to replenish the register with the data obtained, and the analysis of the structure of patients will allow us to expand our understanding of the structure of patients, to form and develop a register of patients with the diagnosis of MM in Uzbekistan.
Keywords: Multiple myeloma, Structure, Distribution of patients, Pathological protein, A-chain, G-chain
Cite this paper: Nasibakhon Xodjiakbarovna Kakhkharova, Abdurakhmon Abdumavlyanovich Kayumov, Structure of Patients with Multiple Myeloma According to the Data of the Republican Specialized Scientific-Practical Medical Center of Hematology, American Journal of Medicine and Medical Sciences, Vol. 12 No. 4, 2022, pp. 386-389. doi: 10.5923/j.ajmms.20221204.04.
Article Outline
1. Introduction
- Currently, multiple myeloma (MM) is defined as a clonal lymphoproliferative disease occurring at the level of pre-B-cell stages of monoclonal development of plasma cell precursors that retain the ability to differentiate to plasmacyte [1,4]. The use of modern polychemotherapy programs allows to achieve clinical improvement, however, according to the data of randomized studies, does not contribute to increase the life expectancy of these patients. This contradiction is largely due to the lack of reliable methods for assessing the prognosis of multiple myeloma in the arsenal of clinicians. [2,3,5,7]. Therefore, the identification of features of the course of the disease associated with life expectancy is an important task. Its solution is of great importance both for practical doctors when working out the therapeutic tactics for a specific patient, and for scientists engaged in assessing the effectiveness of various methods of treatment [6,7,8,10,11].
2. Main Body
2.1. The Purpose of Our Research
- To study the structure and distribution of patients with various forms of multiple myeloma in the Republic of Uzbekistan.
2.2. Material and Methods of Study
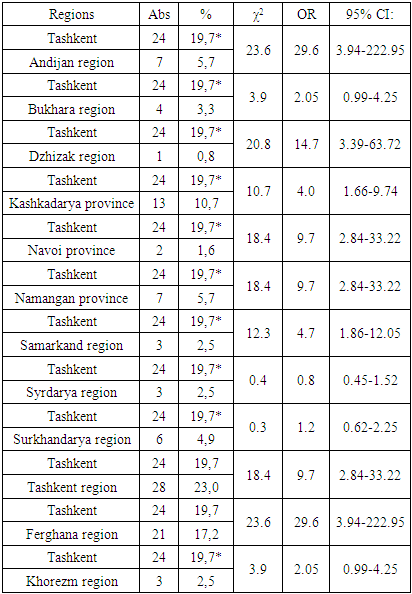
- The study was conducted at the "Hemophilia and Hematopoietic Depression Center" department of the Republican Specialized Scientific-Practical Medical Center of Hematology (RSSPMCH) of the Ministry of Health of the Republic of Uzbekistan. Overall 122 patients with multiple myeloma (MM) were examined, of whom 68 males (55.7%) and 54 females (44.3%) were referred to RSSPMCH. Of these, 119 patients (97.5%) received therapy according to the VCD protocol, 2 patients (1.6%) according to the CVAD protocol, and 1 patient (0.3%) according to the VAD protocol. The sex and age structure of the study sample was examined retrospectively, as well as the distribution of patients in this category according to the regions of treatment. Also a retrospective study of the results of laboratory tests performed on MM patients on the basis of the Laboratory of Medical Genetics (Department of Molecular Medicine and Cellular Technologies) of the RSSPMCH of the Ministry of Health of the Republic of Uzbekistan was carried out. Distribution of different types of chains of pathological proteins characteristic for MM analyzed in blood plasma of patients was studied. Protein composition of patients' blood serum was studied by immunoelectrophoresis on "Interlab pretty" device (Italy) using "Interlab" kits.After the conducted treatment, on the basis of clinical observation, anamnesis collection, questionnaires, in case of necessity examination by specialists (neuropathologist, nephrologist, traumatologist) the complications of the conducted therapy were determined. The revealed manifestations of neuropathy were classified according to their type and severity.Statistical processing of the obtained data was performed using the Internet resource [12] using χ2 test, odds ratio (OR), and confidence interval (95%CI).
2.3. Results of the Study
- A study of the structure of patients with MM was carried out. The study of the distribution of patients by area showed the following picture, presented in Table 1 and Figure 1.
|
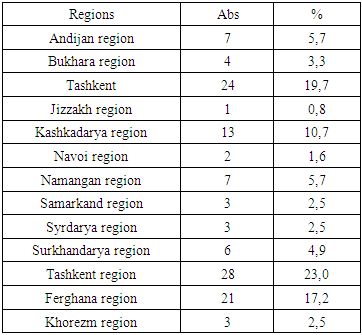
 | Figure 1. Distribution of patients with multiple myeloma by regions of the Republic of Uzbekistan |
|
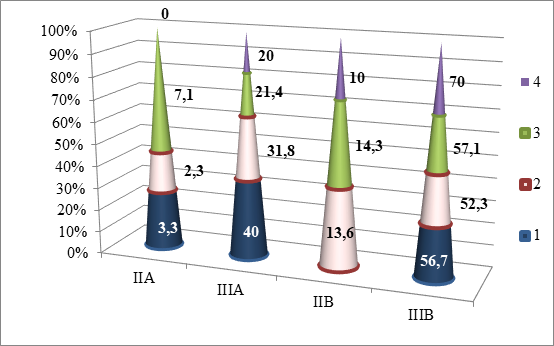 | Figure 2. Distribution of different degrees of neuropathy in different stages of multiple myeloma |
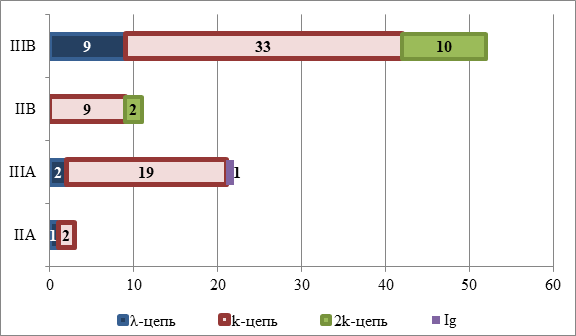 | Figure 3. Distribution of different pathological protein chains in different stages of multiple myeloma |
3. Conclusions
- This work will allow us to replenish the register with the data obtained, and the analysis of the structure of patients will allow us to expand our understanding of the structure of patients, to form and develop a register of patients with the diagnosis of MM in Uzbekistan.
ACKNOWLEDGEMENTS
- We express our gratitude to the Department of Molecular Medicine and Cellular Technologies and the Laboratory of Medical Genetics of the RSNPMCH of the Ministry of Health of the Republic of Uzbekistan. In particular, we thank the Head of the Department, Khamid Yakubovich Karimov, and the Head of the Laboratory of Medical Genetics, Kodirjon Tukhtabaevich Boboev, for their assistance in the organization of the laboratory tests and the laboratory assistant of the Laboratory of Medical Genetics, Liya Kamilovna Mustafina, for conducting the laboratory tests.