Yarmukhamedova Nargiza Anvarovna, Rizaev Jasur Alimdjanovich, Garifulina Lilya Maratovna
Samarkand State Medical Institute, Uzbekistan
Correspondence to: Yarmukhamedova Nargiza Anvarovna, Samarkand State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The bulk of children involved in sports in all return categories had normal physical development (in the range of average z-scores from +1 to -1), while boys had a large percentage of children with reduced body weight at the age of 12, and girls, along with normal development, cases of increased body weight were observed, especially at the age of 13-14 years. When highlighting body types, it was revealed that in the group of boys the muscular body type prevailed, while the thoracic type was the main one in girls. When calculating the tempo somatotype of children with increased physical activity, it was revealed that in both gender groups the macromesosomatic somatotype prevailed, then the micromesosomatic type was noted in frequency of occurrence, while the macrosomatic type prevailed in girls and the microsomatic type in boys.
Keywords:
Athletes, Children, Physical development, Assessment
Cite this paper: Yarmukhamedova Nargiza Anvarovna, Rizaev Jasur Alimdjanovich, Garifulina Lilya Maratovna, Assessment of Physical Development of Young Athletes of Children's and Youth Sports Schools, American Journal of Medicine and Medical Sciences, Vol. 12 No. 4, 2022, pp. 379-385. doi: 10.5923/j.ajmms.20221204.03.
1. Actuality of the Theme
prepubescent and pubertal age is one of the critical stages in human life, since, due to anatomical and physiological features, at this age the body is the most unprotected and vulnerable to the effects of various environmental factors [1]. The selection of children who are able to endure significant psychoemotional and physical loads without harm to their health for 6-10 years and show international-class sports results at the age of 15-18 is an important issue of modern sports medicine.Currently, due to the phenomena of deceleration of physical development in combination with the deterioration of children's health in recent decades, the number of healthy adolescents engaged in sports is decreasing from year to year [2,3]. Coaches have to work with young athletes who already have certain health deviations. Significant physical activity in terms of volume and intensity entails overloads, violations of the harmony of development, lead to the formation of various pathologies. In this regard, the assessment of the physical development of children of prepubescent and pubertal age is relevant in terms of early detection of abnormalities and provision of preventive and health measures for identified abnormalities.The purpose of this study was to assess the physical development of young athletes of children's and youth sports schools in various game sports and athletics of the city of Samarkand.
2. Materials and Methods of Research
803 young athletes aged 11 to 15 years of specialized youth sports schools participated in the research program in various game sports and athletics of the city of Samarkand. The examination of this contingent of young athletes was performed during the medical examination at the city medical physical education dispensary in the period 2018 - 2020.The method of random selection was used in the formation of the sample population. The sample group included children who have been playing sports for more than one year, and representing various sports. At the same time, according to L.P. Matveev's classification (1977) based on the peculiarities of the subject of competitions and the nature of motor activity, children were engaged in the following sports: badminton 1.5% (12), basketball 5.7% (46), volleyball 6.5% (52), handball 8.0% (64), athletics 20.1% (163), table tennis 5% (40), football 20% (161), field hockey 12.7% (23), hand ball 2.9% (23). These sports belong to sports with extremely active motor activity (group 1). Also, the studied sample included children related to the sport, the main content of which was determined by the nature of the abstract-logical beating of the opponent, such as chess 12.2% (98) and checkers 5.2% (42) - Group 2 (Picture 1).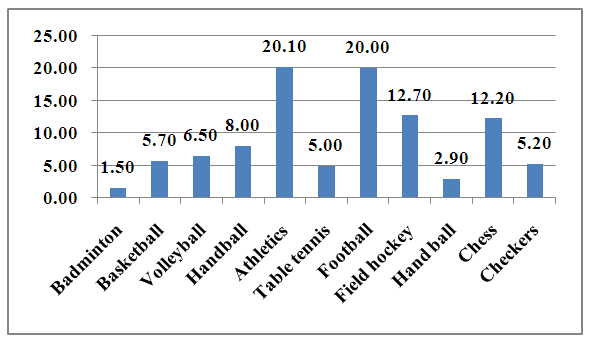 | Picture 1. Distribution of children by sports in the study sample |
The age composition of children was characterized by a sample of prepubescent and pubertal children aged 11 to 15 years, and was distributed as follows, with the largest number of children being pubertal children aged 14 years 52.8% (428). The second age group consisted of children aged 11 years, 21.7% (173), while only 0.5% (4) of children aged 15 years were observed, while children aged 12 and 13 years were almost the same percentage of 12% (97) and 13% (101) (Picture 2). 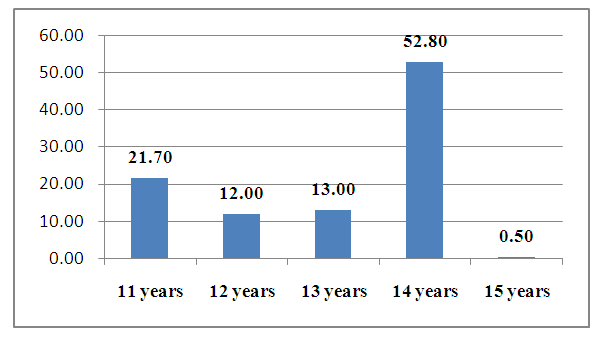 | Picture 2. Distribution of children in the study sample by age |
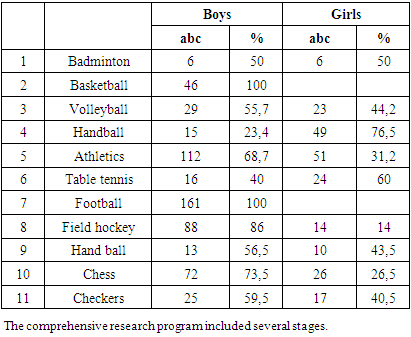
Gender differences showed the absolute number of boys in such sports as football 100% (161), basketball 100% (46), the predominance of boys in volleyball 55.7% (29), athletics 68.7% (68.7), field hockey 86% (88), hand ball 56.5% (13), as well as in chess 77.5% (76) and checkers 54.7% (23). Whereas in handball and table tennis, 49% (76.5) and 60% (24) girls prevailed. You can see the distribution by gender differences in the table.Table 1. Distribution of children in the study sample by gender
 |
| |
|
At the first stage, the somatic status of children from specialized children's and youth sports schools in various game sports and athletics of the city of Samarkand was studied, with the determination of anthropometric data, assessment of the harmony of physical development depending on gender and age.At the second stage of the study, the morbidity of this sample of young athletes was assessed on the basis of an in-depth medical examination, with routine laboratory tests. All information was entered into a specially developed "Map of the study of the morbidity of children and adolescents of children's and youth sports schools according to the data of the appeal". Information from the "Medical control card of the athlete's dispensary observation" (062/U) was also copied into the "Morbidity study card of children and adolescents engaged in children's and youth sports schools". At this stage, a comprehensive assessment of the health status of pupils of sports schools, depending on gender and age, was carried out. The morbidity analysis was carried out in accordance with the International Statistical Classification of Diseases and Health-Related Problems of the 10th revision. A retrospective analysis was also carried out to assess the state of child development and its morbidity in the infancy, early childhood and preschool age.At the third stage, by means of questionnaires and interviews based on a specially developed "Questionnaire for assessing the quality of life of teenagers involved in sports", the image and living conditions of young athletes were studied.At the fourth stage, a study of 225 children with anemia of varying severity was conducted to study the immune status.At the fifth stage of the study, after analyzing the results of studying the state of health and the factors that form it, an organizational experiment was conducted to improve the health of pupils of children's and youth sports schools, for which a set of organizational and therapeutic and preventive measures aimed at reducing morbidity was developed. The organizational experiment included the rehabilitation of young athletes in the conditions of a children's and youth sports school.At the sixth stage, an assessment of the effectiveness of the health measures was carried out. The level and structure of morbidity of athletes were compared before the start of recovery and a year after it (the main group). The control group, selected by the copy-pair method by age, gender and type of sport, consisted of young athletes who did not undergo rehabilitation.
3. The Results of Research
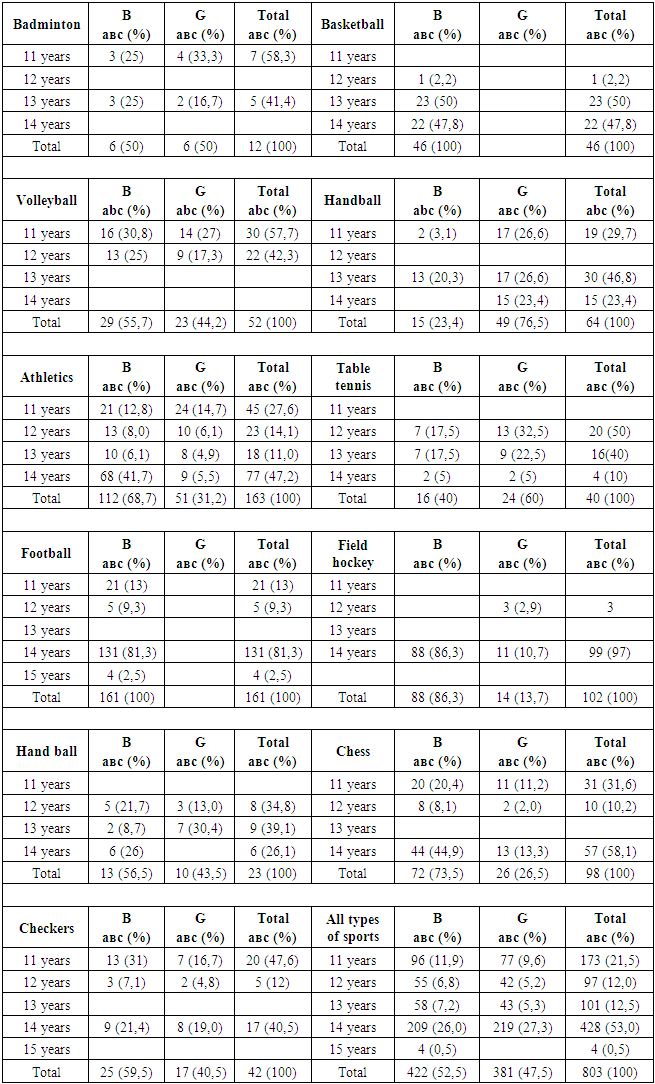
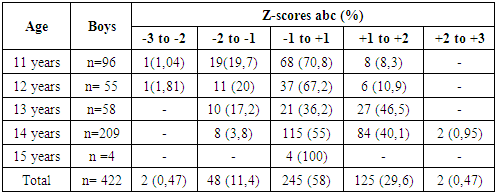
Assessment of physical development is an integral component in the study of the health status of children with increased physical activity due to the fact that it clearly reflects the influence of lifestyle and educational process on the body.The results of in-depth medical examinations served as the basis for assessing the physical development of children and adolescents of children's and youth sports schools. First of all, it was of interest to study the main age composition in groups of children depending on gender and sport. You can see the main data in Table 1.According to the table, each sport was attended by children of different ages, but there were priorities for individual sports. Thus, in the group of children engaged in volleyball, children aged 11 years prevailed - 30 (57.7%), as well as in the group of children engaged in checkers – 20 (47.6%). Children aged 12 were mainly engaged in table tennis 20 (50%). 13-year-olds made up the bulk of those involved in basketball - 23 (50%), and handball - 30 (46.8%) and hand ball - 9 (39.1%).The main part was made up of children aged 14 years, in such sports as athletics - 77 (47.2%), football - 131 (81.3%), field hockey 99 (97%), chess - 57 (58.1%).When studying the physical development of children, we relied on a set of indicators: somatometric, somatoscopic and physiometric, among which the length and weight of the body, the circumference of the chest were subjected to a special assessment. Compliance was carried out in accordance with the standards of the World Health Organization (WHO) ("WHO Growth Reference 2007").Thus, the body mass indicators of the main contingent of children were in the range of average z-scores from +1 to -1, conducting an analysis by age revealed that the largest percentage with these indicators were boys aged 11 years - 68 (70.8%) and 12 years - 37 (67.2%) (Table 2), while boys aged 13 years had z-scores +1 to -1 in just 21 (36.2%), while the bulk of boys had z-scores +1 to +2 - 27 (46.5%), which was most likely associated with the pubertal period and an intense increase in fat mass during this period. At the age of 14, boys' body weight in most cases was within the normal range of 115 (55%), while the number of overweight boys continued to remain at a high level of 84 (40.1%) and there were even cases of obesity in groups of children engaged in chess and checkers - 2 (0.95%). Attention is drawn to the presence of boys with hypotrophy at the age of 11 and 12 years (1.04% and 1.81%). Also, along with cases of obesity in this group, there was a fairly large percentage of children with reduced body weight at the age of 12 years - 11 (20%).Table 2. Age characteristics of children depending on gender and sport
 |
| |
|
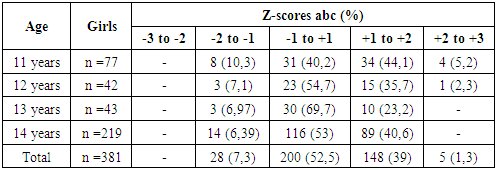
A different picture was observed in the group of girls, so at the age of 11, the z-scores index was in the range of +1 to +2 - 34 (44.1%), i.e. the majority of girls had an increased body weight and even there were cases of overweight - 4 (5.2%) (Table 3).Table 3. Body weight indicators in children (boys) depending on age
 |
| |
|
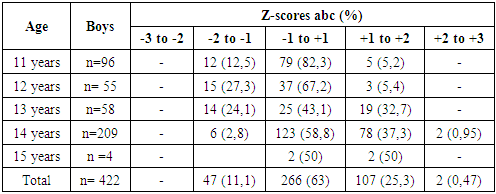
In the process of growing up, the z-scores index was mainly in the average range -1 to +1: at the age of 13, 30 (69.7%), at the age of 14, 116 (53%), while cases of increased body weight were also observed in girls of these age groups: 10 (23.2) girls aged 13 and 89 (40.6%) at the age of 14. If we take in general, the frequency of girls with average weight categories is half of the observations of 200 (52.5%), then there are cases of increased body weight 148 (39%), and reduced body weight 28 (7.3%).As well as body weight, the growth of children aged 11 years was within the average values (Z-scores from -1 to +1 in 79 (82.3%), while 1/3 of children aged 12 years lagged in growth (Z-scores from -2 to -1 in 15 (27.3%), with a high frequency of normal values (Z-scores from -1 to +1 in 37 (67.2%). At the ages of 13 and 14, the growth rates of children accelerated and amounted to Z-scores from +1 to +2 in 19 (32.7%) and 78 (37.3%) (Table 4). Table 4. Body weight indicators in children (girls) depending on age
 |
| |
|
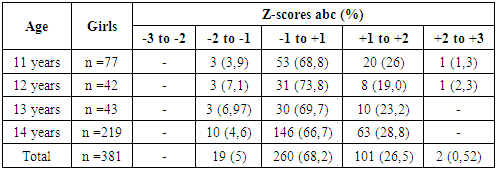
Average growth standards prevailed in girls of all ages (Z-scores from -1 to +1 in 260 out of a total of 381 girls (68.2%), a greater frequency of increased growth was observed at the age of 14 (Z-scores from +1 to +2 in 63 (28.8%). At the same time, the frequency of growth lag was significantly lower compared to the group of boys (Z-scores from -2 to -1 in 19 (%) and 47 (11.1%); p<0.05) (Table 5).Table 5. Growth rates in children (boys) depending on age
 |
| |
|
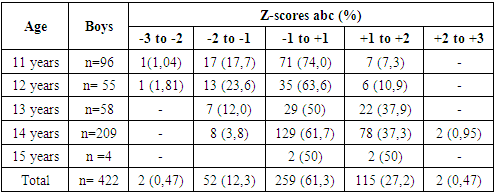
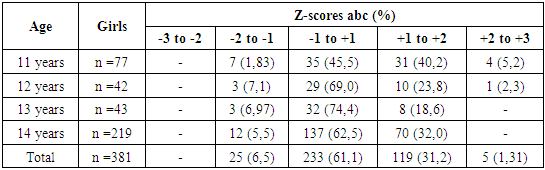
Measurement comparison with percentile diagrams of body weight and height does not always give an objective assessment of the overall physical development of children, in this regard, we have determined the BMI of children involved in sports.For the correct use of BMI in childhood, WHO recommends using a special methodology for assessing physical development in children and adolescents (BMI-for-age 5-19 years) [5,6].The data of the study of boys showed that in all age groups, BMI was in the range of average values (Z-scores from -1 to +1) and was observed on average in 259 children out of 422 (61.3%). Cases of protein-energy deficiency were observed in children aged 11 and 12 years (Z-scores from -3 to -2 in 1 (1.04%) and 1 (1.81%), respectively), as well as underweight children (Z-scores from -2 to -1) in 1/3 of cases in children aged 12 years (13 (23.6%) and in 1/5 of cases in children aged 11 years (17 (17.7%).At the age of 13 and 14, along with the predominance of normal age values of BMI, elevated BMI (Z-scores from +1 to +2) were found at a fairly high frequency in 22 (37.9%) and 78 (37.3% of cases), and there were also cases of overweight (Z-scores from +2 to +3 in 2 children of 14 years (0.95%).When comparing BMI with diagrams for girls, it was revealed that the majority of girls, as well as boys, were in the middle range (Z-scores from -1 to +1) and were observed in 233 girls out of 381 (61.1%), while 1/3 of all observations were girls with BMI in the range of Z-scores from +1 to +2 - 119 out of 381 (31.2%) with slight deviations in each age group (Table 7). It should be noted that the incidence of developmental delays, namely BMI in the range (Z-scores from -2 to -1) was significantly lower compared to boys (25 (6.5%) in girls and 52 (12.3%) in boys; p<0.05). Also, there were no cases of protein-energy deficiency in the girls' group.Table 6. Growth rates in children (girls) depending on age
 |
| |
|
Table 7. BMI indicators in children (boys) depending on age
 |
| |
|
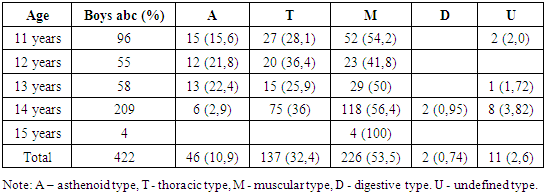
The problem of somatotypes in children remains one of the most controversial and complex in modern constitutionology and the least studied. There are various ideas in the literature about the nature of the factors determining somatotypes and the timing of their formation. The most famous classification of somatotypes of children in our country was proposed by V.G. Shtefko and A.D. Ostrovsky [4].V.G. Shtefko and A.D. Ostrovsky identified four pure body types: asthenoid, thoracic, muscular and digestive. The assessment was made visually, by external signs.Visual assessment revealed that the muscle type of the physique prevailed in the boys' group 226 out of 422 (53.5%), while its greatest frequency was observed in the group of children aged 14 (118 (56.4%) and 11 years (54 (54.2%). The muscular type was characterized by the massiveness of the skeleton with clearly defined distal epiphyses of bones. The thorax is cylindrical, rounded, of the same size along the entire length. The epigastric angle is straight. Back with normally pronounced curves, moderate fat deposition, smoothed bone relief (Table 8).Table 8. BMI indicators in children (boys) depending on age
 |
| |
|
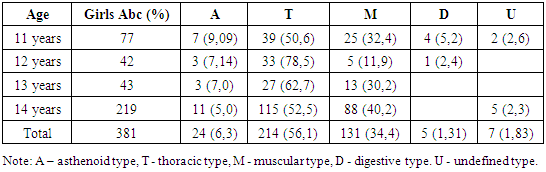
In children aged 12 and 13, in 1/5 of cases, there was an asthenoid body type 12 (21.8%) and 13 (22.4%), characterized by elongated limbs. In this category of children, the chest was elongated, flat, narrowed downwards. The epigastric angle is acute. The back is stooped with sharply protruding shoulder blades, the abdomen is straight. Due to the weakly expressed subcutaneous fat layer, the relief of the shoulder girdle and chest was clearly visible. Cases of undefined physique were noted with the lowest frequency -11 (2.6%).Thoracic type was mainly found in girls of all age groups, its frequency was 214 out of 381 (56.1%). The thoracic type differs from the asthenoid by the development of the thorax, which has a cylindrical shape, slightly flattened, the epigastric angle is straight. The back is normal, sometimes with protruding shoulder blades (Table 9).Table 9. The ratio of the main body types in boys
 |
| |
|
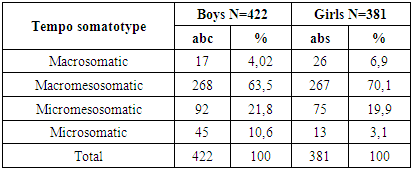
Then, according to the frequency of occurrence in children, muscle type 131 (34.4%) was observed. There were also cases of digestive body type in girls (5 cases (1.31%), which was more than the frequency of occurrence of this body type in the boys' group (2 (0.74%). Cases of indeterminate type were observed in only 7 girls (1.83%).When further assessing the physical development of children engaged in increased physical activity, we calculated the tempo somatotype according to the scheme of P.M. Dorokhov and I.I. Bakhrakh on the basis of centile scales.The results showed that macromesosomatic somatotype prevailed in both gender groups: 268 (63.5%) in boys and 267 (70.1%) in girls. Taking into account the frequency of occurrence, the tempo somatotype was distributed as follows: Micromezosomatic - the second most common 92 (21.8%) in boys and 75 (19.9%) in girls. Macrosomatic type in frequency of occurrence was on the 3rd place in girls 26 (6.9%), while in boys the microsomatic type prevailed on the 3rd place (45 (10.6%), the frequency of which was significantly more often observed in the boys' group (p<0.05) (Table 11).Table 10. The ratio of the main body types in girls
 |
| |
|
Table 11. Distribution of children by tempo somatotype depending on gender
 |
| |
|
4. Conclusions
Thus, the majority of children involved in sports in all return categories had normal physical development (in the range of average z-scores from +1 to -1), while boys had a large percentage of children with reduced body weight at the age of 12 years, and girls, along with normal development, had cases of increased body weight, especially at the age of 13-14 years. When distinguishing body types, it was revealed that in the boys' group, the muscular type of physique prevailed, while the thoracic type was the main one in girls. When calculating the tempo somatotype of children with increased physical activity, it was revealed that the macromesosomatic somatotype prevailed in both gender groups, then the micromesosomatic type was noted in frequency of occurrence, while the macrosomatic type prevailed in girls and the microsomatic type in boys.
References
| [1] | Baranov A.A., Kuchma V.R., Skoblina N.A. Physical development of children and adolescents at the turn of the millennium. Moscow, 2008: 216. |
| [2] | Gelashvili O.A. 1 Hisamov R.R. 2 Shalneva I.R. Physical development of children and adolescents// Modern problems of science and education. - 2018. - No. 3. URL: https://science-education.ru/ru/article/view?id=27656. |
| [3] | Saldan I.P. et al. Modern trends in changes in indicators of physical development of children and adolescents (review article) // Bulletin of Medical Science No. 1 (13) 2019. pp. 14-20. |
| [4] | Tkachuk M.G., Oleinik E.A., Dyusenova A.A. "Sports morphology", 2019. Saint-Petersburg. |
| [5] | Butte N, Garza C, De Onis M. Feasibility of international growth standards for school-aged children and adolescents. The Journal of Nutrition. 2007; 137: 153-157. |
| [6] | De Onis M, Onyango AW, Borghi E, Siyam A. Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization. 2007; 85(9): 660-667. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML