-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(3): 353-357
doi:10.5923/j.ajmms.20221203.26
Received: Mar. 2, 2022; Accepted: Mar. 19, 2022; Published: Mar. 24, 2022

Assessment of the Possibility and Reliability of Laparoscopic Cholecystectomy in Patients with Liver Cirrhosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUrokov Shukhrat Tukhtayevich1, Saidov Ikrom Kokilovich2
1Department of Surgical Diseases and Resuscitation, Bukhara State Medical Institute Named after Abu Ali Ibn Sina
2Department of Surgery №.1, Bukhara Branch of the Republican Scientific Center for Emergency Medical Care
Correspondence to: Saidov Ikrom Kokilovich, Department of Surgery №.1, Bukhara Branch of the Republican Scientific Center for Emergency Medical Care.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Gallstone disease occurs in approximately 1/3 of patients with cirrhosis of the liver (LC). Increased lithogenesis in such patients is presumably associated with an increase in the secretion of unconjugated bilirubin, a decrease in the content of bile acids and phospholipids in bile, and hypomotility of the gallbladder. Gallstones in the gallbladder in patients with cirrhosis rarely migrate, and therefore gallstone disease in most of them is asymptomatic. The need for cholecystectomy in patients with cirrhosis arises, as in patients without cirrhosis, with the appearance of symptoms of biliary colic, acute cholecystitis. It is well known that cirrhosis with portal hypertension increases the risk of intraoperative and postoperative complications in any type of surgical intervention, especially in operations on the biliary tree.
Keywords: Cholelithiasis, Liver cirrhosis, Laparoscopic cholecystectomy
Cite this paper: Urokov Shukhrat Tukhtayevich, Saidov Ikrom Kokilovich, Assessment of the Possibility and Reliability of Laparoscopic Cholecystectomy in Patients with Liver Cirrhosis, American Journal of Medicine and Medical Sciences, Vol. 12 No. 3, 2022, pp. 353-357. doi: 10.5923/j.ajmms.20221203.26.
1. Introduction
- In surgical publications of the 80s of the last century, a high incidence of complications (from 5 to 23%) and deaths (from 7 to 20%) was reported in open surgical interventions on the gallbladder and bile ducts in patients with cirrhosis, with the main causes of adverse outcomes were excessive blood loss, postoperative liver failure and sepsis [6,7]. Initially, cirrhosis with portal hypertension was considered a contraindication for laparoscopic cholecystectomy (LC) due to potential bleeding risks [8]. With the accumulation of experience in laparoscopic surgery, this minimally invasive approach began to be used in a number of difficult situations associated with the gallbladder, including cholelithiasis in patients with cirrhosis. At the same time, recent publications [9] reported a fairly wide range of postoperative complications (6.6-47.3%) and mortality (0-4.3%) in HL in patients with cirrhosis. The first report on the results of HL in patients with cirrhosis was published in 1993 [9]. Subsequently, data from several meta-analyses and randomized controlled trials appeared, confirming the benefits of HL in carefully selected patients with cirrhosis [10-13]. In the present study, we tried, based on our own experience, to assess the feasibility and reliability of HL in the treatment of cholecystolithiasis in patients with cirrhosis.Gallstone disease occurs in approximately 1/3 of patients with liver cirrhosis (LC) [1]. Increased lithogenesis in such patients is presumably associated with an increase in the secretion of unconjugated bilirubin, a decrease in the content of bile acids and phospholipids in bile, and hypomotility of the gallbladder [2]. Gallstones in the gallbladder rarely migrate in patients with cirrhosis, and therefore gallstone disease in most of them is asymptomatic [3]. The need for cholecystectomy in patients with cirrhosis arises, as in patients without cirrhosis, when symptoms of biliary colic, acute cholecystitis appear [4]. It is well known that cirrhosis with portal hypertension increases the risk of intraoperative and postoperative complications in any type of surgical intervention, especially in operations on the biliary tree [5].
2. Material and Methods
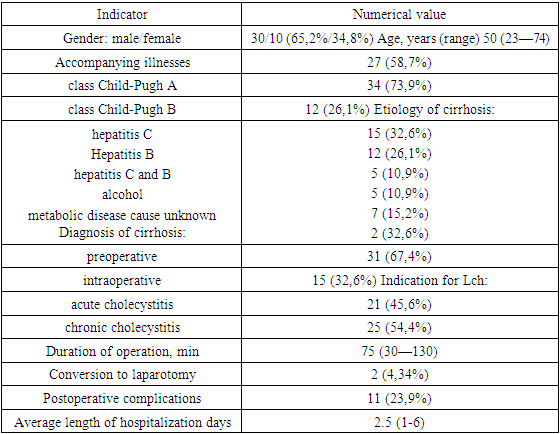
- The case histories of 46 patients with cirrhosis who underwent HL in the clinical bases of the Department of Surgical Diseases and Resuscitation of the Bukhara Medical Institute were subjected to a retrospective analysis for the period from June 2019 to December 2021. The age of patients, gender, etiology of cirrhosis, the nature of gallbladder disease, duration of surgery, intraoperative and postoperative complications, conversion rate to laparotomy, length of hospital stay. There were 30 women (65.2%), men - 16 (34.8%), their mean age was 56.6±12.5 years (range 23-74 years). Hepatitis C was the cause of cirrhosis in 15 (32.6%) patients, hepatitis B in 12 (26%), hepatitis B and C in 5 (10.9%), alcohol abuse in 5 (10.9%), fatty degeneration of the liver - in 7 (15.2%) patients. The etiology of cirrhosis could not be established in 2 patients. The severity of cirrhosis was classified according to Child-Pugh, according to which 34 (73.9%) patients were included in class A, 12 (26.1%) patients were included in class B. There were no patients with decompensated cirrhosis (class C Child—Pugh) in our study. (Table 1).
|
3. Results
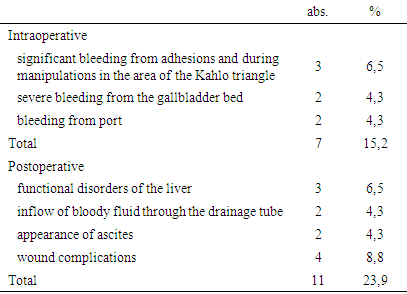
- An attempt at HL, undertaken in 46 patients with cirrhosis, was successfully completed in 44 of them. In 2 cases, a transition to an open operation was required. The cause of conversion in one case was severe bleeding from the bladder bed, which could not be stopped by endoscopic means, in the other case, severe inflammatory infiltration in the bladder neck (Table 2).
|
4. Discussion
- Cholecystectomy is the most common surgical intervention in patients with cirrhosis [15]. It can be dangerous in end-stage liver disease and in portal hypertension due to the greater likelihood of serious complications, especially bleeding and hepatocellular insufficiency. Perhaps for this reason, HL was initially contraindicated in patients with cirrhosis. Later, with the accumulation of experience, as well as the improvement of equipment in laparoscopic surgery, the minimally invasive method gradually replaced open cholecystectomy in this group of patients and became the preferred intervention for cholelithiasis. Recent publications have confirmed the safety and good tolerability of HL in patients with compensated liver cirrhosis [12,14]. The advantages of HL in cirrhosis are a reduction in the incidence of postoperative bleeding, infection, liver failure, and death [10,11]. In this study, we presented our own experience of LC performed in 46 patients with compensated cirrhosis, paying special attention to the indications for this operation, the technique of intervention, and complications. The cause of cirrhosis in most of the patients we observed was hepatitis B and C. (32.6%) cirrhosis of the liver was an unexpected operational finding. The diagnosis of early cirrhosis before surgery for HL is not established, according to some authors, in 18.5-40% of cases [16,17].Ultrasound, as the most accessible non-invasive method, is highly informative in advanced forms of cirrhosis, while its value in the diagnosis of early cirrhosis is still debatable. Perhaps, with the introduction of a relatively new non-invasive method for assessing liver fibrosis, ultrasound elastography (Fibro Scan) will fill the gap in this area. The duration of the operation, the frequency of complications, and the conversion rate for HL in patients with cirrhosis are significantly higher than in patients without this disease [10,11]. The duration of HL in our observations averaged 75 min, which differs little from similar indicators given by other authors [18]. In 4.34% of our observations, a transition to an open operation was required. In recent reports, the conversion rate to laparotomy in HL ranged from 0 to 15.7% [14]. Absolute indications for changing the method of surgery for HL in patients with cirrhosis are bleeding that cannot be stopped by endoscopic means and the risk of manipulations in the hilum of the liver due to varicose vasodilation and anatomical complications.Despite a significant decrease in the frequency of deaths in HL in patients with cirrhosis, postoperative complications in these patients remain at a fairly high level (7.8-35%) [8]. Most often after these operations, liver failure, bleeding, development of ascites, wound infection are noted.In total, we noted complications in 23.9% of patients. In most cases, they were minor, only in one patient the complication turned out to be serious, and a transition to an open operation was required.After surgery, the frequency of deaths in HL in the group of patients with cirrhosis varies, according to the literature, from 0 to 4.3%, averaging 0.45% [14]. Most published studies report no deaths in compensated cirrhosis [19]. There were no deaths in our observations.LH is by far the best option for cirrhosis surgery primarily due to the excellent focal visibility and magnified image provided by the monitor to clearly see the dilated vessels, as well as the availability of appropriate endoscopic hemostatic instruments (ultrasonic scissors, argon plasma coagulator).In addition, with the endoscopic method, the risk of infection of the operating team with hepatitis B and C viruses, which may be in patients with cirrhosis, due to injury with piercing and cutting instruments, is significantly reduced. After HL, there are almost no adhesions in the abdominal cavity, which, probably, may be important in the future for liver transplantation in these patients. At the same time, there are some technical difficulties in LC with CP. The nodularity, hardness of the cirrhotic parenchyma may interfere with the removal of the gallbladder behind the fundus in the cranial direction, which is a necessary maneuver in HL. In addition, in patients with cirrhosis, hypertrophy of the left lobe of the liver, which covers the gate of the liver, is often observed. To eliminate these inconveniences, we, like other authors [8,12], use an additional 5 mm trocar or the introduction of a retractor.Of particular danger in HL in patients with cirrhosis is bleeding from dilated venous collaterals located at the hilum of the liver. The use of ultrasonic scissors allows the dissection to be relatively bloodless. In the absence of confidence in the safety of work in the area of the Kahlo triangle, some authors suggest using options for subtotal cholecystectomy [17].The results of our study and data from other authors show that HL is most suitable for the treatment of symptomatic cholecystolithiasis and acute cholecystitis in patients with mild to moderate cirrhosis (Child-Pugh class A and B).At the same time, cholecystectomy in patients with decompensated cirrhosis (Child-Pugh class C) is a difficult task due to the very high risk of bleeding and liver failure, often leading to an unfavorable outcome [19,20].According to the generally accepted opinion of researchers, elective cholecystectomy in this group of patients should be avoided, and emergency operations should be performed according to emergency indications in the absence of the effect of conservative therapy in progressive cholecystitis [14].Several published studies have shown the effectiveness of percutaneous transhepatic cholecystostomy in such patients [21]. Even attempts were made to endoscopically stent the cystic duct as an alternative to cholecystectomy in patients with cirrhosis [22]. HL in patients with cirrhosis differs in some features that should be taken into account when performing this operation. First, rigorous patient selection is required based on Child-Pugh operative risk assessment or end-stage liver disease (MELD) model. Secondly, a good surgical technique is needed to skillfully circumvent the difficulties and complications to which patients with cirrhosis are especially prone. Thirdly, modern equipment should be used, such as an ultrasonic scalpel or argon plasma coagulator, to minimize bleeding from incised tissues. Finally, great patience is required in this operation in order to successfully complete it laparoscopically, since the transition to open surgery may not always be successful with some complications, such as bleeding due to coagulopathy.
5. Conclusions
- Thus, laparoscopic cholecystectomy can be successfully performed with careful selection of patients with compensated liver cirrhosis. It is advisable to perform this operation by an experienced laparoscopic surgeon in specialized hepatobiliary surgery centers.