-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(3): 268-271
doi:10.5923/j.ajmms.20221203.08
Received: Feb. 20, 2022; Accepted: Mar. 5, 2022; Published: Mar. 9, 2022

Analysis of the Results of Surgical Treatment of Patients with Ventral Hernias and Concomitant Abdominal Pathology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbaniyazov Z. B., Sherbekov U. A., Mardonov B. A.
Department of General Surgery, Samarkand State Medical Institute, Samarkand, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

According to the World Health Organization (Geneva, 2017) anterior abdominal wall hernias combined with concomitant abdominal diseases are among the most common surgical conditions, occurring in 3-7% of the population, predominantly affecting the working-age population [5,14]. According to the literature, 15-20% of patients who have undergone herniotomy undergo repeated surgical interventions for other surgical diseases in the years following the operation [2,12]. This determines the relevance of the problem of simultaneous operations. Attention should be paid to the irrationality of performing only herniotomy for ventral hernia (HH) if the patient has concomitant abdominal disease. In the case of herniotomy alone, reoperation for concomitant abdominal pathology often negates the results of hernioplasty [1,10,11]. According to F.G. Nazirov (2018), simultaneous operations on the abdominal wall and abdominal organs nowadays increase the complexity of the intervention, but it reduces the treatment period, reduces the risk of possible complications after herniotomy in the form of associated diseases due to additional anesthesia and emotional distress related to the need for repeated intervention [4,9]. In patients with hernias, the most frequently identified pathology is in the gallbladder, in women - in the pelvic organs, in the abdominal cavity - adhesions, chronic and subacute intestinal obstruction, etc [3,8,13]. Approaches to performing simultaneous interventions in patients with hernias have their own peculiarities, since the location of the organs with pathology may not coincide with the localization of the hernia. The presence of adhesions, adhesive intestinal obstruction and fistulas located at different levels of the gastrointestinal tract may pose special problems [15]. This requires a detailed surgical technique at the herniotomy stage, the intra-abdominal stage and the closure of the abdominal cavity.
Keywords: Ventral hernia, Simultaneous pathology, Surgical correction
Cite this paper: Kurbaniyazov Z. B., Sherbekov U. A., Mardonov B. A., Analysis of the Results of Surgical Treatment of Patients with Ventral Hernias and Concomitant Abdominal Pathology, American Journal of Medicine and Medical Sciences, Vol. 12 No. 3, 2022, pp. 268-271. doi: 10.5923/j.ajmms.20221203.08.
1. Introduction
- The study was based on 235 ventral hernia patients operated on in the surgical department of the 1st Clinic of Samarkand State Medical Institute during the period from 2014 to 2021. The patients were conventionally divided into two groups: 124 (52.8%) patients underwent only hernioplasty; they constituted the comparison group. 111 (47.2%) patients underwent simultaneous interventions for abdominal cavity diseases requiring surgical correction and with ventral hernia being the main surgical pathology. At the time of the surgery the patients were aged from 16 to 78 years (mean age 49,4 ± 11,8 years). Females predominated among the patients - 54.8%, men - 45.2%. Investigation methods complied with clinical standards recommended by WHO and MOH: patients were evaluated for their general condition; comorbidities were identified and their compensation degree was determined; general clinical laboratory examination was carried out; ultrasound examination, MSCT, endoscopic studies were carried out.Hernias of medial localization (MWR) made up the most numerous group - in 184 (93.4%) patients. Lateral abdominal hernias (LWR) were in (6.6%) of patients. The ventral hernia was small in 10.2% of patients, medium in 25.4%, large in 35%, and huge in 29.4%. 88.3% of patients were admitted with postoperative ventral hernia, and 11.7% of patients were admitted with hernias of large and huge sizes, i.e., the overwhelming contingent - 127 (64.5%) were patients with postoperative hernias of median localization.Altogether 178 combined pathologies of abdominal organs requiring surgical correction were revealed in 111 patients of the main group (28 patients - 2 combined pathologies, 6 patients - 3). More frequently in patients with ventral hernias were revealed cholelithiasis - 36 (32,4%), pelvic pelvic pathology in women - 31 (27,9%), adhesions of the abdominal cavity - 67 (60,4%), obesity III - IV stage, sagging abdomen - 32 (28,8%), etc.The summary data of the treatment of patients with hernias showed that the number of patients requiring simultaneous interventions increased with the hernia size. For small hernias (W1), 16 (15.3%) concomitant pathologies were identified, for W2, 31 (29.8%), for W3, 62 (59.6%), and for W4, 69 (66.3%).Simultaneous pathology at the preoperative stage was diagnosed in 74.6% of patients, intraoperatively - in 5.4%.
2. Material and Methods
- In 65.4% of the main patients and in 61.3% of the control group there was concomitant somatic pathology which required perioperative preparation: cardiovascular diseases in 40.6% of the examined patients, respiratory diseases in 11.8%, diabetes mellitus in 4.3%, III-IV degree obesity in 28.7% and others. - in 28.7%, etc. According to the ASA classification, 52.8% of patients corresponded to the 1st class, 36.5% - to the 2nd class, and 10.7% - to the 3rd class. In assessing the operative-anesthetic risk we took into account not only the presence of somatic pathology, but also its clinical and laboratory signs. The choice of surgical access was primarily based on the location of the hernia gate, the location of the organ with concomitant pathology in the abdominal cavity areas. In this regard, a schematic dystopia was developed, i.e. the localization of the hernial defect on the abdominal wall and the location of concomitant pathology in the abdominal cavity. The nature of the hernial bulge was assessed according to the classification of Chevrel J.P. and Rath A.M. and the location of concomitant pathology was guided by the topographic division of the abdominal cavity into 9 regions.In the main group of patients (25.2%) the surgical stage of abdominal surgical pathology correction was carried out using the laparoscopic access; in 23 of them the hernioplasty stage was also performed using the endovideosurgical method. In 83 patients (74.8%) all stages of surgery were performed using a single herniolaparotomy access.At the same time the nature of the performed simultaneous surgeries were as follows: cholecystectomy for cholelithiasis - 36 (including LCE - 16), visceralysis for abdominal adhesions and chronic intestinal obstruction - 67, cystectomy from the liver - 6, Pancreas - 2, ovaries - 9 (laparoscopic cystectomy - 3), uterine amputation or extirpation - 35, and dissection of the cutaneous subcutaneous flap of the anterior abdominal wall - 32.Then we proceeded to the main stage of the operation - the liquidation of hernial defect. The choice of hernioplasty in both study groups was differentiated. Tension methods of alloplasty: - implantation of endoprosthesis "onlay" with suturing of the defect was performed in 47,1% of the main group and 49,5% - of the control group of patients.Non-tension methods: implantation of endoprosthesis "onlay" without suturing of the defect in 42,3% and 40,9%; implantation of endoprosthesis "onlay" without suturing of the defect with Ramirez mobilization of rectus abdominis muscle vaginas in 10,6% and 9,7% of patients in the main and control groups correspondingly. Intraabdominal endoprosthesis implantation was performed laparoscopically in 23 (20.7%) patients of the main group. Dermatolipidectomy along the line fringing the Castanares herniated bulge was performed in 26.4% of patients who had concomitant pathology in the form of II-III degree obesity and a sagging abdomen after the completion of anterior abdominal wall plasty (Fig. 1).
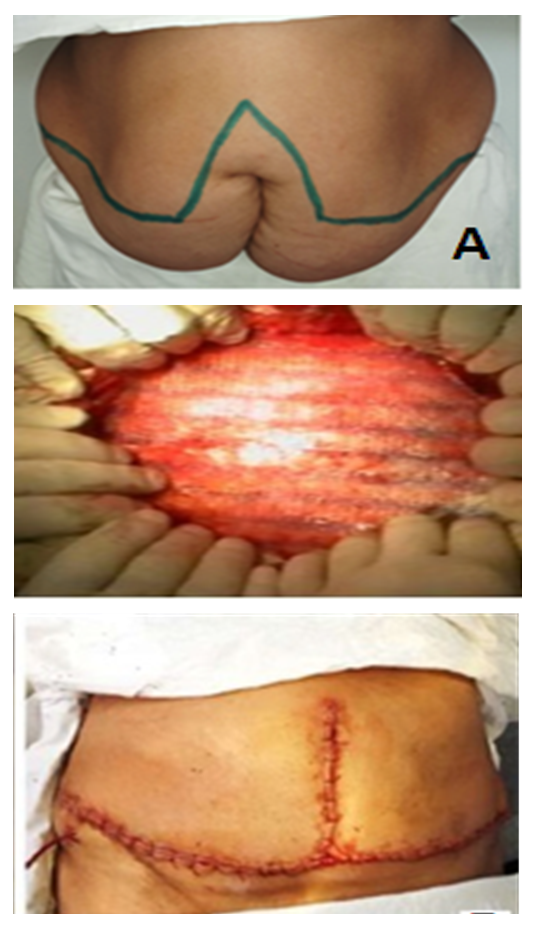 | Figure 1. Stages of hernialloplasty with abdominoplasty: - incision line framing the hernial bulge according to Castanares (A); - implantation of endoprosthesis (B); - anterior abdominal wall at the end of the operation (C) |
3. Results and Discussion
- The following parameters were used as the main criteria to assess the effectiveness of the treatment results of the patients in the compared groups: abdominal complications of the early postoperative period; extra-abdominal complications of the early postoperative period; wound complications in the early postoperative period (Fig. 2).
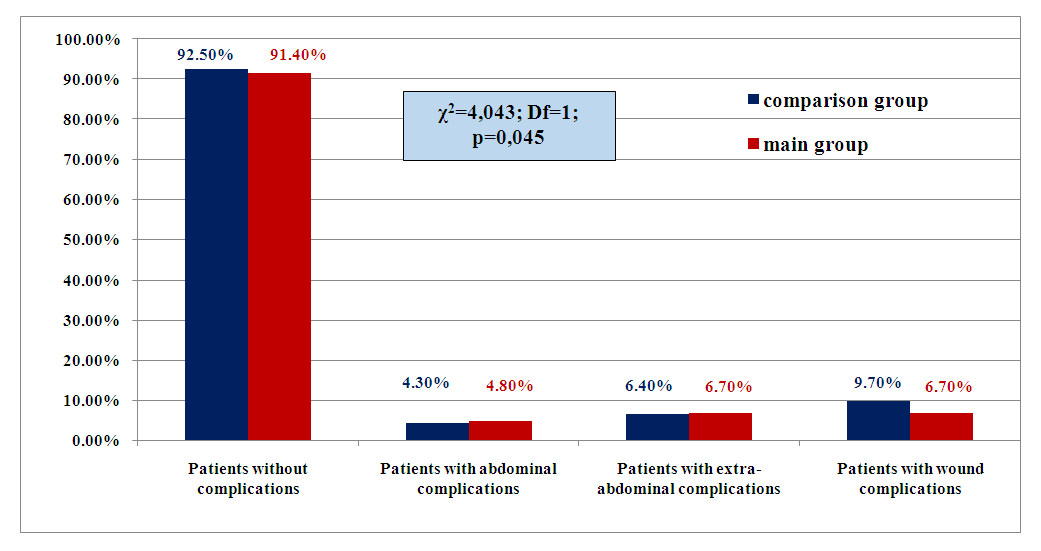 | Figure 2. Frequency of complications in the compared groups in the immediate postoperative period |
4. Conclusions
- 1. According to our data the simultaneous abdominal cavity pathology requiring surgical correction in ventral hernias was 47,2%; biliary stone disease - 32,4%, pelvic organs pathology in women - 27,9%, adhesions of the abdominal cavity - 60,4%, obesity III - IV degree sagging abdomen - 28,8% were revealed most frequently in patients with ventral hernias. Simultaneous pathology was diagnosed at the preoperative stage in 74.6%, intraoperatively - in 25.4% of cases. The number of patients requiring simultaneous interventions increased with increasing hernia size: at W3 - 59.6%, at W4 - 66.3%. 2. In the main group 28 patients (25.2%) underwent laparoscopic access surgery to correct surgical pathology of abdominal cavity; in 23 of them the hernioplasty stage was also performed using endovideosurgical method. In 83 patients (74.8%) all stages of surgery were performed using a single herniolaparotomy access. 3. The choice of hernioplasty should be differentiated. Tension methods of alloplasty: onlay endoprosthesis implantation with suturing of the defect was performed in 47.1% of patients of the main group and 49.5% of the control group. Non-tensioned ways: endoprosthesis onlay implantation without suturing the defect - 42,3% and 40,9% respectively; endoprosthesis onlay implantation without suturing the defect with mobilization of rectus abdominis vaginis according to Ramirez - 10,6% and 9,7%. Dermatolipidectomy was performed in 26.4% of patients with concomitant pathology in the form of II-III degree obesity and saggy abdomen after the anterior abdominal wall plasty. 4. Complications in the immediate postoperative period in the compared groups were comparable: abdominal complications were observed in 4,8 and 4,3% of the operated patients, respectively; extra-abdominal complications (bronchopulmonary and cardiovascular) - in 5,7 and 6,4%; compartment syndrome - in 0,9 and 1,1%; wound complications - in 9,7 and 6,7%. Lethality in the main group and in the comparison group was 0.9 and 1.1%, respectively. 5. Performance of the simultaneous stage of surgery in general had no negative influence on the results of surgical treatment of patients with ventral hernia and simultaneous pathology of the abdominal cavity organs. The elimination of several diseases in a single anesthesia and surgical intervention dictates the need to perform simultaneous surgeries.