-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(3): 265-267
doi:10.5923/j.ajmms.20221203.07
Received: Feb. 22, 2022; Accepted: Mar. 6, 2022; Published: Mar. 9, 2022

Method for Transvaginal Hysterectomy in Recurrent and Complicated Prolapse of the Uterus and Vaginal Walls
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNegmadzhanov Bakhodur Boltaevich, Shavkatov Khasan Shavkatovich, Nasimova Nigina Rustamovna
Department of Gynecology №2, Samarkand State Medical Institute, Samarkand, Uzbekistan
Correspondence to: Shavkatov Khasan Shavkatovich, Department of Gynecology №2, Samarkand State Medical Institute, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article analyzes the features of the surgical treatment of recurrent prolapse of the uterus and vaginal walls after various operations. The study involved 53 patients with internal genital prolapse after various operations, the average age in the 1st group was 58.9 years, in the 2nd group - 46.8 years. All women undergo generally accepted mandatory general clinical and gynecological research methods. We studied the methods of surgical tactics of genital prolapse after surgery.
Keywords: Genital prolapse, Ventricular fixation, Transvaginal hysterectomy, Rectocele, Cystocele
Cite this paper: Negmadzhanov Bakhodur Boltaevich, Shavkatov Khasan Shavkatovich, Nasimova Nigina Rustamovna, Method for Transvaginal Hysterectomy in Recurrent and Complicated Prolapse of the Uterus and Vaginal Walls, American Journal of Medicine and Medical Sciences, Vol. 12 No. 3, 2022, pp. 265-267. doi: 10.5923/j.ajmms.20221203.07.
Article Outline
1. Introduction
- Pelvic organ prolapse (POP) - a syndrome of pelvic floor and organ prolapsed of the small pelvis alone or in combination, which has an extremely negative impact on the quality of life of patients. According to world data, from 2.9 to 53% of women report certain manifestations of POP [1]. Up to 47% of patients with pelvic organ prolapse are women of working age. According to the Women's Health Initiative Study, among 16,616 perimenopausal women, the incidence of uterine prolapse was 14.2%, cystocele - 34.3%, rectocele -18.6% [2]. In most cases, PTO is practically asymptomatic, which indicates its greater prevalence in the population [3].A particular problem is PG after hysterectomy. According to the literature, the incidence of vaginal dome prolapse after hysterectomy reaches 43%. [14]. The disease has a wide age range, in addition, in recent years there has been a noticeable "rejuvenation" of this pathology, an increase in the number of complicated and recurrent forms. To reduce the recurrence rate after traditional vaginal correction, operating gynecologists have begun using mesh implants to improve support for pelvic floor structures. The high efficiency of using synthetic implants in the correction of inguinal hernia, abdominal gastropexy, etc. has long been known [4]. Current data on pelvic floor surgery indicate that the use of a mesh implant in pelvic floor surgery has not only positive results but also specific complications. Operations are often associated with risk, which has been actively discussed recently [5,6,]. Specific complications arising after correction using the so-called mesh (ang, mesh) include protrusion of the mesh into the vagina (erosion) [7], into the bladder, intestines, the development of infection, the appearance of pain, dyspareunia, urinary disorders, and other pelvic dysfunctions. To extremely formidable infectious complications include isolated cases of pelvic abscesses and fasciitis, rectovaginal and vesicovaginal fistulas, as well as the formation of rough scars in the implantation zone. These rare complications occur in less than 3% of patients but can lead to a significant reduction in quality of life. According to the literature, POP recurrence most often occurs in women after cystocele correction [8,9], as well as in patients with POP stage III (cysto- or rectocele) [2,3].The problem does not lose its relevance. Due to changes in the demographic situation, a progressive increase in the number of patients with pelvic floor dysfunction can be expected, because women of advanced and senile age are the fastest-growing segment of the population. In addition, there is an increase in the number of complicated and recurrent forms of this pathology.This indicates the need to study the reproductive behavior of women after surgical treatment of genital prolapse using highly effective contraceptive methods.Purpose of the study: To improve the effectiveness of a new modification of surgical treatment in patients with genital prolapse of varying severity and to prevent recurrence of the disease.
2. Materials and Methods of Research
- A survey of 53 patients was conducted, of which 21 patients were operated on for genital prolapse, and 32 were observed for the first time with PG from different clinics, who were routinely admitted to the gynecological department of the maternity complex No. 3 of the city of Samarkand in the period from 2017 to 2020.All examined were divided into 2 groups: (39.6%) women who were operated on for genital prolapse and came with complications, who were the comparison group, and (60.4%) women who, during surgical treatment of genital prolapse, used new modifications of surgical correction - the main group.The average age in the 1st group was 58.9 years, in the 2nd group - 46.8 years. All women under observation were studied clinical and anamnestic indicators of women. A general examination, external and internal obstetric examination, clinical blood and urine tests were carried out, the group and Rh belonging of the blood were determined, the blood was examined for the Wasserman reaction, bacterioscopic and bacteriological examination of the contents of the cervix and vagina, urinalysis according to Nechiporenko. During the study, the main group (61.9%) of patients was diagnosed with various forms of inflammatory processes (cervicitis, endocervicitis ...), although the symptoms of PG dominated the clinical picture. It should be noted that in our patients of the 1st group with recurrent prolapse, the relapse period is 1-4 years.The quality of life of patients with genital prolapse and surgical correction with a new modification was assessed 3 years after surgical treatment.
3. Results of the Study
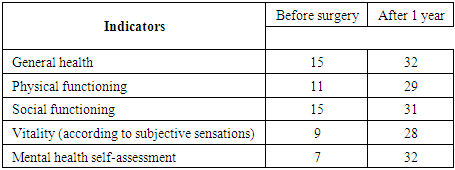
- The choice of tactics of management, volume and access of surgical treatment of patients with female genital prolapse, as well as an objective assessment of the effectiveness of its results and postoperative rehabilitation was carried out based on anamnesis data, clinical, laboratory, ultrasound and complex urodynamic methods of research. Regardless of volume and access, in the operation aimed at the elimination of prolapse of the genital organs, including those complicated by urinary incontinence, as the main or one of the components included the correction of the incompetence of the muscles of the pelvic floor with the obligatory narrowing of the genital gap.In the main group, 32 patients underwent surgical correction, with a new modification. After a transvaginal hysterectomy, the vaginal stump to the abdominal cavity is left open by suturing the pelvic peritoneum together with the ligament stumps to the proximal wall of the vagina with “x” shaped vinyl sutures, without periodization, which ensures reliable hemostasis and adequate drainage of the small pelvis, which guarantees the prevention of postoperative stump and infiltrate, inflammation of the pelvic peritoneum and improves the conditions for tissue repair and scar formation, as well as the recurrence of prolapse of the walls of the vagina. In this case, enterocele does not develop. Next, we perform colpoperineolevathoroplasty according to the technique. At the control examination after 12 months, the height and depth of the vagina, the condition of the scars, the tone of the vaginal muscles, urinary function, and the condition of the cervix were assessed.For a comparative assessment of the long-term results of surgical treatment of OVPO in patients of the main group, urination control was performed, the volume of the cervical stump was determined, the total length of the vagina, genital fissure, and height of the vagina were measured.According to the examination after 12 months, there was normal architectonics of the perineum and vagina, the stump of the cervix, which looked healthy in all patients.This behavior of the woman was also explained by the fear of "disrupting the effect of surgical treatment." There were significantly fewer negative emotions during intimacy. Women noted an increase in the frequency of experienced orgasms, arousal by a sexual partner, and sexual desire. All these changes led to an increase in satisfaction with sexual life, which indicates a positive impact on the quality of life.Indicators of women with genital prolapse in the main group after surgery with a new modification.
 We observed unfavorable outcomes of OVPO correction after a year in 1 patient with recurrent prolapse of the anterior vaginal wall of the 1st degree, which did not require surgical correction.
We observed unfavorable outcomes of OVPO correction after a year in 1 patient with recurrent prolapse of the anterior vaginal wall of the 1st degree, which did not require surgical correction.4. Conclusions
- Features of the postoperative course and long-term results of surgical correction of genital prolapse indicate the high efficiency of the proposed method of surgical correction of genital prolapse and ensured a 1.5-fold reduction in the risk of infiltration and divergence of postoperative sutures, a reduction in the length of stay of patients in the hospital by 1.45 days and the risk of developing relapses of the disease in the long-term follow-up period by 1.6-2.8 times.