-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(3): 243-250
doi:10.5923/j.ajmms.20221203.02
Received: Feb. 11, 2022; Accepted: Mar. 4, 2022; Published: Mar. 9, 2022

Visual Anatomical Deviations of the External Genitals in Girls. Current State of the Issue (Literature Review)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. I. Zokirov, B. B. Negmadzhanov
Ministry of Health of the Republic of Uzbekistan, Samarkand State Medical Institute, Department of Obstetrics and Gynecology No. 2, Samarkand, Uzbekistan
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Visual anatomical (phenotypic) deviations of the external genitalia present significant difficulties for both patients and their parents, as well as medical workers who, in connection with their professional duties, advise and provide medical care, since there are many contradictions in management tactics. Visual anatomical (phenotypic) deviations of the external genitalia are any visible to the eye - ad oculus deviations from the norm of the structure of the external genitalia, such as the degree of development of the clitoris, the structure of the large and small labia, the type of introitus, the location of the external opening of the urethra.
Keywords: He location of the external opening of the urethra
Cite this paper: F. I. Zokirov, B. B. Negmadzhanov, Visual Anatomical Deviations of the External Genitals in Girls. Current State of the Issue (Literature Review), American Journal of Medicine and Medical Sciences, Vol. 12 No. 3, 2022, pp. 243-250. doi: 10.5923/j.ajmms.20221203.02.
Article Outline
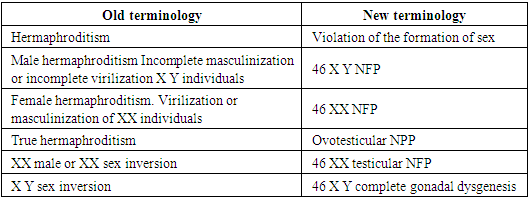
- Classification of anomalies of the female genital organs: in surveys, the classification of diseases of the reproductive system is still discussed at numerous forums, congresses. But unfortunately, there is still no consensus on this matter, and various sources or authors’ own systematizations are still used in scientific research and practice, which do not always cover the entire spectrum of causes [2].Given the above, professors A.B. Okulov and B.B. Negmadzhanov (2000) [2] systematized lesions of the reproductive system requiring surgical treatment in accordance with critical remarks and modern requirements for pediatric surgical care. A distinctive feature of this classification is the coverage of diseases of the reproductive organs of both girls and boys.According to this systematization, lesions of the reproductive system are divided into 2 large groups of congenital diseases and acquired diseases. Below is an abbreviated form of this systematization.Classification of surgical diseases of the reproductive system [2].1. Congenital Diseases1.1. Complex (“classic”) disorders of sexual differentiation1.1.1. Gonad forms1.1.1.1. Female type of external genitalia1.1.1.2. Mixed (gender indefinite) type of external genitalia1.1.1.3. Male type of external genital organs1.1.2. Extragonadal forms (due to a genetic defect in androgen reception or high levels of extragonadal androgens)1.1.2.1. Female type of external genitalia1.1.2.2. Mixed (gender indefinite) type of external genitalia1.1.3. Rare forms of disorders of sexual differentiation1.1.3.1. Female type of external genitalia1.1.3.2. Mixed (gender indefinite) type of external genitalia1.1.3.3. Male type of external genitalia1.2. Small (“non-classical”) forms of violation of sexual differentiation1.2.1. Female type of external genitalia1.2.2. Mixed (gender indefinite) type of external genitalia1.2.3. Male type of external genital organs1.2.4. Breast lesions1.2.4.1. Female phenotype1.2.4.2. Male phenotype2. Acquired Diseases (postnatal impairment of sexual differentiation)2.1. Gonadal forms2.1.1. Female type of external genitalia2.1.2. Male type of external genital organs2.2. Extragonadal forms2.2.1. Female type of external genitalia2.2.2. Male type of external genital organs2.3. Rare forms2.3.1. Female and male phenotypes2.4. Changes in the external genitalia due to previous diseases and injuries2.4.1. Female type of external genitalia2.4.2. Male type of external genital organs2.5. Iatrogenic lesions of the organs of the reproductive system2.5.1. Female phenotype2.5.2. Male phenotype2.6. Acute diseases of the reproductive organs2.6.1. Female phenotype2.6.2. Male phenotypeAs can be seen, the above classification deals with disorders associated with the urogenital sinus. Separately from the above, anomalies in the development of internal genital organs in women, the so-called. anomalies in the development of derivatives of the Mullerian ducts. The Müllerian ducts, being the primordial rudiments of the female reproductive tract, differentiate to form the fallopian tubes, uterus, cervix, and upper aspects of the vagina.To systematize the anomalies of this group, the classification of the American Society for Reproductive Medicine (formerly the American Fertility Society) is most widely used, based on the classification of V. Buttram and W. Gibbons ( Buttram V. 1983) [9], which combined the degree of developmental disorders with clinical manifestations. This ASRM classification includes 7 classes, and is given below [46]:Class I. _ Partial (hypoplasia) or complete agenesis of the Müllerian ducts:I.A. _ – vaginalI.B. _ - cervicalI.V. _ - uterineI.G. _ - pipeI.D. _ - combinedClass II. Unicorn uterus:II.A. - with a rudimentary horn with an endometrial cavity:II.A.1. - communicating with the second hornII.A.1. - not communicating with the second hornII.B. - with a rudimentary horn without an endometrial cavityII.B. - without rudimentary hornClass III. Doubling uterus:Class IV. Bicornuate uterus:IV.A. _ – with full separation (with two cervixes)IV.B. – with partial separation (with one cervix)Class V. _ Uterus with septum:V.A. _ - full baffleV.B. _ - incomplete partitionClass VI. Arcuate (saddle) uterusClass VII. Uterus with intracavitary changes (T-shaped, strands in the uterine cavity, expansion of the lower three-quarters of the uterus - the consequences of intrauterine exposure to diethylstilbestrol, turinal).Along with the above, there are also so-called small forms of lesions of the organs of the reproductive system, which are not included in the above classifications. These include atresia of the hymen, synechia of small genitals.Atresia of the hymenHymen serves as the boundary between the internal and external genitalia in the female. The hymen itself develops as a result of the proliferation of synovaginal bulbs and the vaginal plate (urogenital tubercle), the perforation of which occurs before or immediately after birth. Atresia of the hymen is observed when the complete sewage of this "plate" is disrupted and is the extreme degree of various disorders of the sewage process, such as annular narrowing (hymen anularis), cloisonne hymen (hymen septus), trellised (hymen cribriformis), high hymen (hymen altus) as well as differences in the rigidity and/or elasticity of the hymen tissue [2,22].The etiological factors leading to atresia of the hymen are not known today, and according to some authors, it occurs sporadically. But in the literature there are data on family cases, and often it occurs together with other anomalies of the genitourinary system [17,43].Epidemiology: Being the most common and distal form of obstructive pathology of the female genital organs, ADP, according to different authors, occurs with a frequency of 1 per 10,000 to 1 per 1,000 people [22]. Diagnosis: It is not uncommon for neonates with hymenal atresia to develop mucocolpos shortly after birth under the influence of maternal estrogen.Diagnosis of mucocolpos is not difficult, and during a routine gynecological examination in the genital area, a bulging of the stretched hymen can be detected. A whitish turbid mass shines through it [2]. Despite the fact that mucocolpos is a benign congenital pathology, late diagnosis can lead to severe morbidity and additional medical interventions [39]. Thus, based on the foregoing, we can say that today, along with gynecological and / or recto -abdominal examination, ultrasound of the pelvic organs is the only method for diagnosing mucocolpos, in which a formation in the small pelvis can be detected.Clinic: due to bursting, a formation that causes severe pain, children are often restless, poorly fed, they have frequent painful urination. In severe cases, the mucocolpos becomes so large that it may give the impression of a small pelvis. In 37-60% of these patients, urinary retention and constipation are observed. In some, urinary retention is so severe that bilateral hydronephrosis can occur, leading to acute kidney injury and fatal sepsis [29,36].Treatment: To date, the only treatment for atresia of the hymen is surgical treatment - dissection of the hymen (hymenotomy or hymenectomy). Currently, the classical method is widely used throughout the world using a cruciform incision of the hymen, in which, after evacuation of the contents, 4 edges of the excised hymen are sutured to the vaginal mucosa using absorbable suture material to achieve hemostasis and prevent secondary closure of the hymenal opening [22,38,44].This method, despite a good surgical outcome, has a huge drawback, since when sewing the edges of the hymen to the vaginal mucosa, the integrity of the hymen is often violated. In addition, when making an incision and suturing, there is a high risk of injury to both the hymenal ring and the urethra, and the risk of re-closure of the hymenal opening is also high. Thus, according to Lee et al. (2019), who conducted a comprehensive systematic review of the literature with the number of patients of 236 people, complications such as re-closure of the hymenal opening, cicatricial stenosis of the vaginal inlet, the need for repeated surgical intervention, etc. were observed in 15 patients (6.6%), while a satisfactory outcome was observed only in almost 60% of patients. In 75 patients (31.8%), the treatment outcome was unknown [29].Taking into account the fact that an intact hymen is a sign of virginity, this disadvantage is unacceptable in many social cultures and religions, including in Uzbekistan. Therefore, to date, there are several descriptions of the technique of surgical treatment of hymenal atresia with preservation of the integrity of the hymen in the literature. For example, Acar Ali et al (2007) in their work described the method of surgical treatment of 65 patients with preservation of the integrity of the hymen. After the central puncture of the hymen and expansion, they evacuated the contents and, to prevent re-fusion, inserted a Foley catheter into the incision and inflated the cuff to 10 cm3. The catheter was left in place for 2 weeks and an estrogen-containing ointment was applied to the hymen for 2 weeks. A single dose of antibiotics was given prophylactically. According to the authors, the result was satisfactory in 100% of cases, the hymen remained open and intact [3]. Unlike Acar Ali, Temizkan O. _ et al (2012), use the method of excision of the central part of the hymen without the use of a Foley catheter and estrogen -containing ointments. Although they used this method in only 2 cases, they report satisfactory postoperative results [45].C deserves interest. Cetin et al., 2016, in which 15 patients with hymen atresia were operated on by circular excision of the central part of the hymen using an electrocoagulator. The results according to the authors were satisfactory in 100% of cases. No complications or relapses were observed [11]. Also found in the literature is the work of M. Basaran et al. (2009), where they describe 2 cases of treatment of hymen atresia complicated by hematocolpos with a vertical incision in the hymen and multiple sutures on the edges of the hymen to prevent reoccurrence. The authors assure the integrity of the hymen after such treatment and recommend surgical treatment as a hymen-preserving method [6].To date, in addition to the studies described above, there are also many modifications of surgical techniques in the literature using laser or electrosurgery or traditional methods that preserve the integrity of the hymen.Fusion of the labia minoraUnions of the labia minora or the so-called synechia are fibrous fusion of the labia minora, which completely or partially closes the entrance to the vagina, and in severe cases to the urethra. Typically, fusion begins at the posterior commissure and continues anteriorly to the clitoris.Etiology: The cause of the appearance of synechia is considered to be a hypoestrogenic state, therefore this pathology does not occur after the onset of menarche, when the synthesis of sex hormones (estrogens) begins. Also in newborns, due to the intake of maternal estrogen with breast milk, this pathology does not occur. However, a study by Ca ğ lar M. _ K. _ et al. in 2007, showed that there are no statistically significant differences in the level of estradiol in children with synechia and children from the control group [10]. Also, according to a number of authors, inflammatory processes (vulvovaginitis), mechanical irritation and tissue trauma (use of diapers, synthetic underwear, hematomas and injuries of the external genitalia) play an important role in the development of synechia [31]. All this is apparently due to the fact that, in a state of hypoestrogenism, inflammatory processes proceed faster and without any protective mechanisms of the body. There is hyperactivation of macrophages, which are responsible for the destruction of cells at the site of inflammation. In response, the body tries to restore damaged epithelial tissues - collagen production is underway.Epidemiology: According to the literature, synechia of the labia minora occurs in 1.8% of girls, with a peak incidence at the age of 13-23 months [31]. And according to Dowlut - McElroy T et al (2019), can occur with a frequency of up to 22% in prepubertal girls, as many cases go unnoticed due to the absence of symptoms [13].Diagnosis: According to the literature, in more than 35% of cases of synechia remain asymptomatic [33,42] and the discovery of this pathology by chance by parents during hygienic procedures entails great psychological discomfort in the family. Typically, such patients are subjected to many unnecessary examinations and wandering around doctors, which in turn add to the psychological burden. Synechia can be easily diagnosed during routine examination. In children under 18 months of age, examination is best done in the frog-leg position, while in children over 18 months in the dorsal lithotomy position. Usually the fusion starts from the posterior commissure and goes anteriorly towards the clitoris for some distance. In severe cases, synechia completely block the entrance to the vagina and urethra. There is no need for special research methods for the diagnosis of synechia [28].Clinic: As it was said in 35% of cases of synechia are asymptomatic [33,42]. When synechia completely block the entrance to the vagina and sometimes the urethra begins to flow into the vagina, symptoms of urinary obstruction appear, leakage of urine after the act of urination, the so-called post- urethral leakage of urine or vaginal urination, in severe cases up to acute urinary retention and dysuric symptoms [42]. In 20-40% of patients, there are symptoms of urinary tract infections, hematuria, symptoms of vulvovaginitis due to urinary retention [28,33].Treatment: Some authors recommend expectant management until symptom onset [5], while others recommend immediate treatment to prevent symptom onset [33,42]. To date, the method of choice for the treatment of synechia in asymptomatic course is the use of estrogen -containing ointments. Many authors recommend using the surgical manual method of treatment if conservative therapy is ineffective and/or if there are dense adhesions, if synechia is symptomatic, and if parents refuse conservative therapy [4,15,33,42].According to various authors, the effectiveness of local estrogen -containing is 15-100% [4,27,33,42], and the recurrence rate varies within 11-41% [15,33,42,47]. And with manual treatment, the recurrence rate is 15% [33,42], i.e. and with conservative and surgical tactics, relapses are observed. With each relapse, the adhesions become even more dense and extended.The main disadvantage of manual separation of adhesions is the painfulness of the procedure, so it is recommended to perform under general anesthesia [33]. The disadvantages and side effects of local estrogen -containing ointments are local irritant effect, vulvar hyperpigmentation, engorgement and enlargement of the mammary glands, and often spotting from the genital tract [13,28].Recently, there have been reports in the literature about the use of betamethasone -containing ointments as an alternative method of treatment. The authors report no side effects, satisfactory results up to 90% and, of course, the availability of the latter in terms of the financial capabilities of patients [16,32,35].Studies using betamethasone -containing ointments in the treatment of synechia are encouraging, but studies published in the literature are insufficient and require further study.Sex formation disordersSex formation disorders, formerly known as hermaphroditism, intersex conditions, bisexuality, are a group of congenital diseases characterized by a clinical and biochemical discrepancy between genetic, gonadal, and phenotypic sex [30].In 2006, at an international conference on disorders of sex formation, organized by the Lawson Society for Pediatric Endocrinology Wilkins, together with the European Society of Pediatric Endocrinologists, adopted a consensus to revise the terminology and nomenclature of hermaphroditism. It was proposed to replace both the term hermaphroditism itself, which sounds offensive to patients, and the indication of gender in the diagnosis, i.e. male or female hermaphroditism. The use of the term " Disorders of Sex Development " (D S D), in the Russian version "disorders of sex development" (NFP) is recommended. Thus. NFP is a congenital condition caused by a chromosomal, gonadal, or somatic disorder of sex formation [14,30].
|
|
