-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2022; 12(1): 46-52
doi:10.5923/j.ajmms.20221201.09
Received: Dec. 28, 2021; Accepted: Jan. 22, 2022; Published: Jan. 24, 2022

Improvement of Medical Aid for Endocrinological Patients in the Conditions of a Family Polyclinic and a Rural Medical Center
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLO. F. Yusupov1, N. J. Ermatov2
1Independent Researcher, Tashkent Medical Academy, Tashkent, Uzbekistan
2Doctor of Medical Sciences, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: N. J. Ermatov, Doctor of Medical Sciences, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article is devoted to general practitioners working in family polyclinics (FP) and rural medical centers (RMC), who do not possess sufficiently enough the skills of timely detection of risk factors and borderline conditions of diabetes mellitus and iodine deficiency diseases, at the initial preclinical stages, the diagnosis of which is carried out at screening methods, which is usually performed using cheap, simple, non-invasive diagnostic procedures with high sensitivity.
Keywords: Risk factors, Obesity, Impaired glucose tolerance, Diabetes mellitus, Iodine deficiency states, Screening, Follow-up
Cite this paper: O. F. Yusupov, N. J. Ermatov, Improvement of Medical Aid for Endocrinological Patients in the Conditions of a Family Polyclinic and a Rural Medical Center, American Journal of Medicine and Medical Sciences, Vol. 12 No. 1, 2022, pp. 46-52. doi: 10.5923/j.ajmms.20221201.09.
Article Outline
1. Introduction
- Reforming of healthcare is one of the important directions of state policy, - said the President of the Republic of Uzbekistan (RU), at a meeting with health care specialists on January 5, 2017. In his speech, he focused on issues related to the activities of FP / RMCs, which are sufficiently equipped with the necessary treatment and diagnostic resources. Indeed, today all the conditions have been created for conducting primary medical consultation in order to solve the problems of the population, to identify more effectively risk factors for non-communicable diseases, including diabetes mellitus and iodine deficiency conditions.
2. The Main Results and Findings
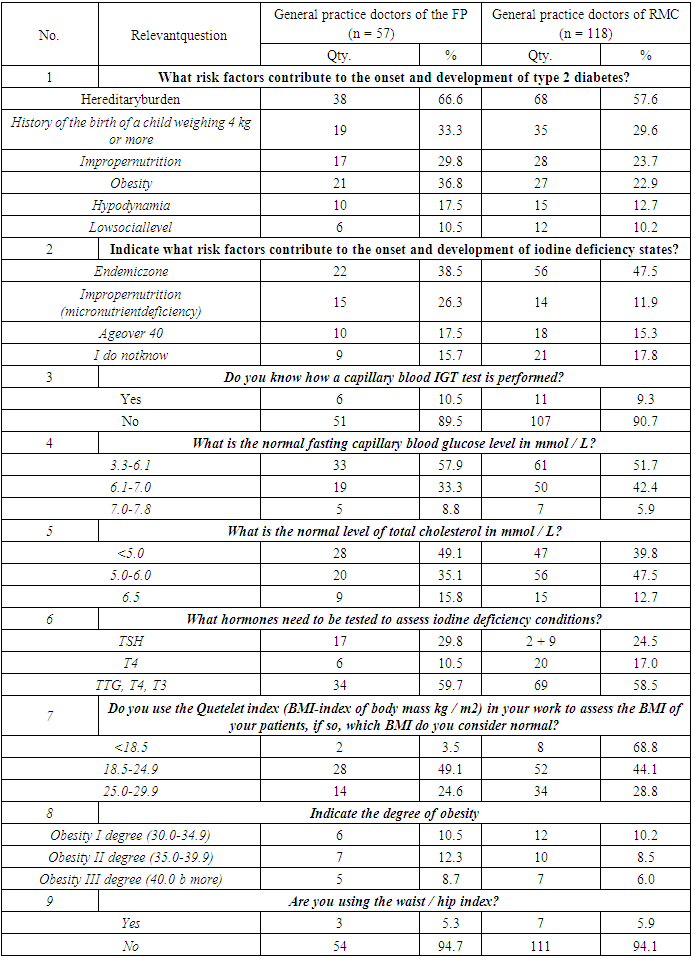
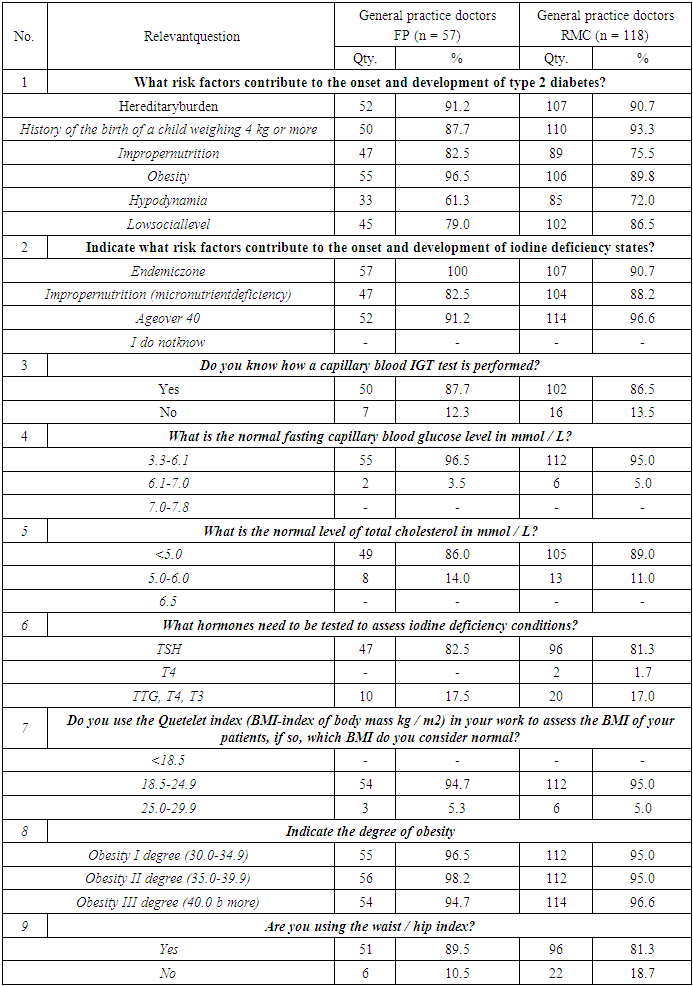
- In the "Action Strategy in five priority areas of development of the Republic of Uzbekistan for 2017-2021", the tasks have been defined on "improvement the quality and availability of medical and social medical aid for patients with endocrine pathology" on the basis of high modern technologies, wider implementation of comprehensive measures to reduce the mortality of the population from complications of endocrinological diseases.Increase in the effectiveness of primary and secondary prevention and treatment of type 2 diabetes in the conditions of FP/RMC must be noted with particular importance.It should be noted that endocrine diseases at the present stage are a serious health problem in many countries of the world; their relevance is due to their social significance and prevalence among population. The leading positions among endocrine pathology are occupied by disorders of carbohydrate metabolism (impaired fasting glycemia, impaired glucose tolerance (IGT), diabetes mellitus (DM) types 1 and 2), then - thyroid diseases (autoimmune thyroiditis, diffuse toxic goiter, nodular goiter, etc.) [1,2,3,4,5].Disorders of carbohydrate metabolism, including pre-diabetic conditions and type 2 diabetes itself, especially in association with obesity are the most common in the world. Every year the number of patients with pathology of carbohydrate metabolism increases. Considering the prevalence of IGT on average in 20-25% of the population, as a rule, detected during routine examination for some other reason, the annual transformation in 1.5-10% of IGT into type 2 DM, latent course (a long period of imaginary well-being) development diabetes is becoming an epidemic [6,7,8,9,10]. According to the forecasts of the World Health Organization (WHO), by 2025 the number of patients with type 2 diabetes in the world will double and reach 333 million people. The DM problem is a priority in almost all developed countries of the world and in Uzbekistan is no exception.Lack of iodine in the environment leads to the development of iodine deficiency diseases, which, according to WHO, are the most common endocrine pathology in the world, 1570 million people (30% of the world's population) are at risk of developing iodine deficiency diseases, including more than 500 million people living in the regions with severe iodine deficiency and a high prevalence of endemic goiter [11].In Uzbekistan, according to an endocrinological study carried out in 2004, among all endocrine pathology, thyroid diseases turned out to be the most common. Their share is 69.8%, including diffuse endemic goiter - 61.3%, other non-toxic forms of goiter -2.8%. hypothyroidism - 1.6 / o. hyperthyroidism. 2.7%. tirsoilite - 1.2%, diabetes mellitus - 19.0%, etc. [12,13].Iodine deficiency conditions are an important medical and social problem. In areas with a pronounced iodine deficiency, perinatal mortality, the incidence of still births and congenital malformations are significantly increased [14,15,16,17,18].To study the problem of protecting the health of endocrine patients, particularly of type 2 DM devoted a large number of studies by local and foreign authors. At the same time, there is an insufficient level of availability of high-quality endocrinological care for rural residents, which determines the need for further scientific and practical development of issues of organizing medical care for patients with type 2 diabetes, living both in the city and in the countryside. This led to the relevance, scientific novelty and predictive value of this study.This study, to a certain extent, serves to fulfill the tasks provided for in the decree of the President of the Republic of Uzbekistan Presidential Decree (PD) No. -4947 "On the strategy of actions in five priority areas of development of the Republic of Uzbekistan for 2017-2021." dated February 7, 2017; Resolutions Presidential Order (PO)-3071 "On measures for the further development of the provision of specialized medical care to the population of the Republic of Uzbekistan in 2017-2021." of June 20, 2017, as well as other regulatory documents adopted in this area. The ongoing health care reforms in the republic, in particular the organization of FP / RMC, have created a real opportunity for primary and secondary prevention of all diseases, including endocrine diseases.Considering the often very poor clinical picture of type 2 diabetesand sometimes complete absence of symptoms, in a significant part of patients by the time of diagnosis, the duration of the disease is 7-12 years, while a high percentage of vascular complications are revealed. A UK. PDS prospective study conducted in the UK showed that 50% of patients with newly diagnosed type 2 diabetes already have signs of vascular lesions, which are the main cause of disability and mortality. According to the City Diabetes Center of St. Petersburg, during routine, non-screening detection of type 2 diabetes, in 57.1% cases patients had macrovascular diseases, and 54.4% had microvascular complications, and their later stages were recorded more often. Considering such high prevalence of chronic vascular complications by the time type 2 DM is diagnosed, the interest of doctors and healthcare providers in programs for the early detection of diabetic patients and those at increased risk of developing of it is growing.The purpose of the study there was an assessment of the quality of medical care in primary health care, provided by general practitioners to patients with endocrine pathology, with the development of measures to improve its quality. In accordance with the set goal of the study, the following tasks were solved:1. To study the incidence and prevalence of obesity in urban and rural populations.2. To assess the quality of medical care provided to patients with endemic goiter and hypothyroidism in the conditions of FP / RMC.3. To study the state of screening and control of type 2 DM in the conditions of FP / RMC and the possibilities of a general practitioner in the implementation of preventive measures.4. To study the satisfaction of the population with the quality of medical care for patients with endocrine pathology in the conditions of FP / RMC.5. To develop an electronic algorithm for early diagnosis with personal dynamic monitoring of patients with endocrine pathology and improve the system of measures to combat risk factors in primary health care.Interviewed general practitioners of the FP in Tashkent and RMCs of the Tashkent, Fergana, Namangan, Syrdarya, Surkhandarya and Kashkadarya regions, who underwent 10-month retraining courses at educational medical centers No. 1,2 at the Tashkent Medical Academy in the 2011/12 academic year. Before and after training on the skills of early detection of endocrine diseases (impaired fasting glycemia, impaired glucose tolerance (IGT), type 2 DM, autoimmune thyroiditis, diffuse toxic goiter, nodular goiter, etc.), 175 doctors were questioned. Among them, 57 (32.8%) doctors worked in the FP in Tashkent, 118 (67.2%) - in the RMC. After receiving instructions, groups of trained doctors filled out questionnaires anonymously. In the next stages of the study, a survey, clinical examination and the necessary laboratory and instrumental examinations of the adult population was carried outin four areasfromFP/RMCs in total in the amount of 2610 people. 800 people among them were from the FP No. 37, located in Chilanzar district, city of Tashkent; in the FP No. 38 – 510 people respectively; in the Tashkent region of the Kibray district in the RMC "Dzhambul" * 510 people; in the Fergana region of the Uchkuprikdistict in the RMC "Yakkamulla" - 790, respectively. An algorithm for an electronic program aimed for an early diagnosis of prediabetes and type 2 DM has been developed at primary health care level.General practitioners working in FP / RMCs are not sufficiently skilled in the timely identification of risk factors and borderline conditions for diabetes mellitus and iodine deficiency diseases, at the initial preclinical stages, diagnosed by screening, which is usually carried out using cheap, simple, non-invasive diagnostic procedures with high sensitivity.A certificate of 12.10.2018 (No. DGU 05726) was received on the official registration of the algorithm of the electronic program for an early diagnosis of prediabetes and type 2 diabetes mellitus in primary health care level.In our study, with the help of the questionnaire that we have compiled, we interviewed doctors of the FP in Tashkent and doctors of RMCs of Tashkent, Fergana, Namangan, Syrdarya, Surkhandarya and Kashkadarya regions, who underwent 10-month retraining courses at educational and medical centers No. 1, 2 at the Tashkent Medical Academy in the 2011/12 academic year. Before and after training on the skills of early detection of endocrine diseases (impaired fasting glycemia, IGT, type 2 diabetes, autoimmune thyroiditis, diffuse toxic goiter, nodular goiter, etc.), 175 doctors were questioned. When analyzing the questionnaires, the main indicators indicated in Table 1 were assessed.
|
 Date: "____"____________20___yearFULL NAME. patient:Gender: male ... female ...1. Patient's age:Under 45... 0 points45-54 years old... 1 point 55-64 years old... 2 points Over 65 years old ... 3 points2. Features of the profession:Physical inactivity and intellectual-emotional load - no ... 0 pointPhysical inactivity and intellectual-emotional load- yes ... 1 point3. Hereditary burden of diabetes mellitus (DM)No ... 0pointYes ... 1 point (grandmother-grandfather, aunts-uncles, cousins and brothers)Yes ... 2 points (dad-mom, siblings and brother)4. Hereditary burden but CVD (HD, IHD) and obesity or the presence of chronic pancreatitis, CVD and their complications in the patient himself (HD, IHD, MI, MI, CHF)No ... 0 point. Yes ... 1 point5. If the gender is female, it is necessary to determine whether the patient has a history of giving birth to a child with a large weight (4 kg or more ...)No ...0 point.Yes ... 1 point6. Obesity according to the WHO classification 1997 Determination of body mass index (BMI)No ... 0 point (BMI from 18.5-24.9)Yes ... 1 point (before obesity - BMI 25.0-29.9)Yes ... 2 points (grade I obesity - BMI 30.0-34.9)Yes ... 3 points (obesity II degree - BMI 35.0 39.9)Yes ... 4 points (grade III obesity - BMI 40 or more)7. Abdominal obesity (abdominal circumference in cm. At the level of the navel)• Amongwomen:No ...0 point (up to 80 cm.)Yes ... 1 point (80-88 cm)Yes ... 2 point (more than 88 cm)• Inmen:No ...0 point (up to 94 cm.)Yes ... 1 point (94-102 cm)Yes ... 2 point (more than 102 cm)8. SmokingNo ... 0 pt. Yes ... 1 point9. Alcohol abuse No ... Oh score"Onholidays" ... 1pointChronicalcoholdependence ... 2 points10. Bloodpressure (BP)Norm ... 0 pointAH 1 degree ... 1 pointAH grade 2 ... 2 pointsAH grade 3 ... 3 points11. TinaPowerRationalnutrition .. 0 pointOvereating ... 1 pointAbuse of easily digestible carbohydrates ... 2 pointAbuse of easily digestible carbohydrates and foods from animal fats ... 3 points12. Fasting blood glucose (blood vein) (WHO 1999)Norm (4.0-6.1 mmol / L) ... 0 point Increased (from 6.1 to 7.0 mmol / L) ... 1 point Increased (from 7 mmol / L to 11.0 mmol, / L) ... 2 points13. Blood glucose 2 hours after meals (WHO, 1999)Norm ... o point (up to 7.8 mmol / l)Impaired glucose tolerance (IGT) ... 1 point (from 7.8-11.1 mmol / L) Diabetes mellitus ... 3 points (11.1 mmol / L and above)14. Lipid spectrum (European recommendations III revision 2003)• Total cholesterol norm (<5.0 mmol / L) ... 0 point • Total cholesterol increased (> 5.0 mmol / L) ... 1 point• LDL cholesterol norm (<3.0 mmol / l) ... 0 point • LDL cholesterol (> 3.0 mmol / L) ... 1 point• HDL cholesterol (> 1.0 mmol / L in men;> 1.2 mmol / L in women) ... 0 point• HDL cholesterol is lowered (<1.0 mmol / L in men; <1.2 mmol / L in women) ... 1 point• TG norm (<1.77 mmol / L) ... 0 point• TG increased (> 1.77 mmol / L) ... 1 point15. SecondarysymptomsofdiabetesmellitusPolydipsia (thirst): No ... 0 point Yes ... 1 pointPolyphagia (increased appetite): No ... 0 point Yes ... 1 pointPolyuria (diabetes): No ... 0 point Yes ... 1 point16. Glycatedhemoglobin (WHO, 2011)Upto 4.0 - 5.6% 0 pointFrom 5.7 - 6.4% 1 point1.5% ormore .... 2 points
Date: "____"____________20___yearFULL NAME. patient:Gender: male ... female ...1. Patient's age:Under 45... 0 points45-54 years old... 1 point 55-64 years old... 2 points Over 65 years old ... 3 points2. Features of the profession:Physical inactivity and intellectual-emotional load - no ... 0 pointPhysical inactivity and intellectual-emotional load- yes ... 1 point3. Hereditary burden of diabetes mellitus (DM)No ... 0pointYes ... 1 point (grandmother-grandfather, aunts-uncles, cousins and brothers)Yes ... 2 points (dad-mom, siblings and brother)4. Hereditary burden but CVD (HD, IHD) and obesity or the presence of chronic pancreatitis, CVD and their complications in the patient himself (HD, IHD, MI, MI, CHF)No ... 0 point. Yes ... 1 point5. If the gender is female, it is necessary to determine whether the patient has a history of giving birth to a child with a large weight (4 kg or more ...)No ...0 point.Yes ... 1 point6. Obesity according to the WHO classification 1997 Determination of body mass index (BMI)No ... 0 point (BMI from 18.5-24.9)Yes ... 1 point (before obesity - BMI 25.0-29.9)Yes ... 2 points (grade I obesity - BMI 30.0-34.9)Yes ... 3 points (obesity II degree - BMI 35.0 39.9)Yes ... 4 points (grade III obesity - BMI 40 or more)7. Abdominal obesity (abdominal circumference in cm. At the level of the navel)• Amongwomen:No ...0 point (up to 80 cm.)Yes ... 1 point (80-88 cm)Yes ... 2 point (more than 88 cm)• Inmen:No ...0 point (up to 94 cm.)Yes ... 1 point (94-102 cm)Yes ... 2 point (more than 102 cm)8. SmokingNo ... 0 pt. Yes ... 1 point9. Alcohol abuse No ... Oh score"Onholidays" ... 1pointChronicalcoholdependence ... 2 points10. Bloodpressure (BP)Norm ... 0 pointAH 1 degree ... 1 pointAH grade 2 ... 2 pointsAH grade 3 ... 3 points11. TinaPowerRationalnutrition .. 0 pointOvereating ... 1 pointAbuse of easily digestible carbohydrates ... 2 pointAbuse of easily digestible carbohydrates and foods from animal fats ... 3 points12. Fasting blood glucose (blood vein) (WHO 1999)Norm (4.0-6.1 mmol / L) ... 0 point Increased (from 6.1 to 7.0 mmol / L) ... 1 point Increased (from 7 mmol / L to 11.0 mmol, / L) ... 2 points13. Blood glucose 2 hours after meals (WHO, 1999)Norm ... o point (up to 7.8 mmol / l)Impaired glucose tolerance (IGT) ... 1 point (from 7.8-11.1 mmol / L) Diabetes mellitus ... 3 points (11.1 mmol / L and above)14. Lipid spectrum (European recommendations III revision 2003)• Total cholesterol norm (<5.0 mmol / L) ... 0 point • Total cholesterol increased (> 5.0 mmol / L) ... 1 point• LDL cholesterol norm (<3.0 mmol / l) ... 0 point • LDL cholesterol (> 3.0 mmol / L) ... 1 point• HDL cholesterol (> 1.0 mmol / L in men;> 1.2 mmol / L in women) ... 0 point• HDL cholesterol is lowered (<1.0 mmol / L in men; <1.2 mmol / L in women) ... 1 point• TG norm (<1.77 mmol / L) ... 0 point• TG increased (> 1.77 mmol / L) ... 1 point15. SecondarysymptomsofdiabetesmellitusPolydipsia (thirst): No ... 0 point Yes ... 1 pointPolyphagia (increased appetite): No ... 0 point Yes ... 1 pointPolyuria (diabetes): No ... 0 point Yes ... 1 point16. Glycatedhemoglobin (WHO, 2011)Upto 4.0 - 5.6% 0 pointFrom 5.7 - 6.4% 1 point1.5% ormore .... 2 points
|
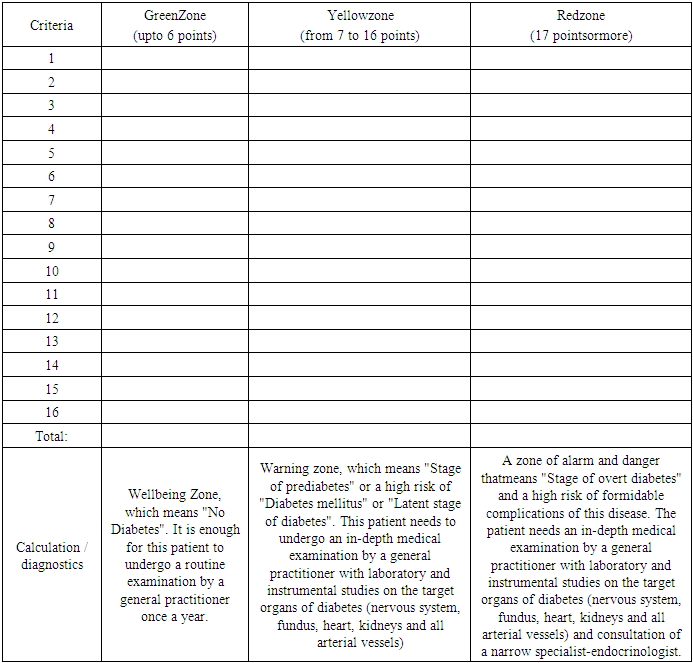
3. Interpretation of the Results Obtained
- 1. If the patient's scores correspond to the “Green Zone” (6 points), this is the well-being zone, which means “No Diabetes”. It is enough for this patient to undergo a routine examination by a general practitioner once a year.2. If the patient's scores correspond to the "Yellow zone" (from 6 to 17 points), this is a warning zone, which means "Stage of prediabetes" or a high risk of "Diabetes mellitus" or "Latent stage of diabetes". This patient needs to undergo an in-depth medical examination by a general practitioner with laboratory and instrumental studies on the target organs of diabetes (nervous system, fundus, heart, kidneys and all arterial vessels).3. If the patient's scores correspond to the "Red Zone" (17 or more points), this is an alert/danger zone, which means "Stage of overt diabetes" and a high risk of severe complications of this disease. This patient needs an in-depth medical examination by a general practitioner with laboratory and instrumental studies on the target organs of diabetes (nervous system, fundus, heart, kidneys and all arterial vessels) and consultation of a narrow specialist - an endocrinologist.
4. Conclusions
- Training of general practitioners in the skills of early detection of type 2 diabetes and iodine-deficiency states contributes to the prevention of formidable complications, timely control of diseases and is one of the effective methods in the complex treatment of endocrine patients.General practitioners are not sufficiently skilled in the early detection of risk factors for endocrine pathology; poorly proficient in screening methods for type 2 diabetes and iodine deficiency diseases. The proposed algorithm of the electronic program for early diagnosis of prediabetes and type 2 diabetes mellitus to the existing system of diabetological care for the urban and rural population of Uzbekistan will improve the quality of early detection of the disease. In addition, using this technology for early diagnosis, it is possible to personalize the tactics of managing and treating patients with type 2 diabetes in the conditions of FP / RMC, preventing formidable complications of this disease, improving the quality and life expectancy of the population.
References
| [1] | Balabolkin M.I. Solved and unresolved issues of endemic goiter and iodine deficiency states // Problems of endocrinology. -2005. -№4. -p.31 -37. |
| [2] | Gaskov A.Yu., Savchenko M.F..Yushkov N.N. Features of the development of iodine deficiency states in children living in conditions of environmental pollution with fluoride compounds // Hygiene and sanitation. - 2005. - No. 6. - p. 53-55. |
| [3] | Egoshina L.V. Endocrinological service // Coll. scientific works, - Yoshkar-Ola, 1994. -p. 21-23. |
| [4] | Fields. PP, Hendrich C.E. The role of thyroid hormones in prenatal and neonatal neurological development - current perspectives // Endocrine Reviews. -1993. -V.14 - No. 1. -p. 94-103. |
| [5] | Harris K.B., Pass K.A. Increase in congenital hypothyroidism in New York state and in the United States // Mol. Genet. Metab. -2007. -N91. -p. 268-77. |
| [6] | Alberti George Consensus IDF no Prevention of type 2 diabetes // Diabetes. Lifestyle. - 2008. - N1. - p. 79-82. |
| [7] | Demidova T. Yu. Difficulties and prospects of obesity treatment // Diabetes. Lifestyle. - 2008. - N1. - p. 76-78. |
| [8] | Shestakova M.V. About the tasks of the world and Russian // Dianovosti. 2007. -№2.-p.3. |
| [9] | Ford E., Williamson D 'Liu S. Weight change and diabetes incidence findings from a national cohort of US adults // Am. J. Epidemiol. - 1997 Vol. 146.-p. 214-222. |
| [10] | Meta-analysis subclinical thyroid dysfunction and the risk l "* r coronars heart disease and mortal it) N. Ochs. To Auer. B.C. Baueret al // Ann Intern. Med - 2008. - Vol. 148. - p. 832-845. |
| [11] | The Colorado thyroid disease prevalence study // G.J. Canaris. N.R. Maniwitz, G. Mayor, E.G. Ridgway // Arch. Intern. Med. -2000. -Vol.160. -p.526-534. |
| [12] | Mukhamedov T.M. Clinical examination of patients with diabetes mellitus in the Republic of Uzbekistan II News. doctor's general practice. - 2001 - No. 2. - p. 31-33. |
| [13] | Mukhammedov T.M., Abdujabborova D.Kh. The frequency of endocrine pathology among the population of Uzbekistan for the last decade // Problems of biology and medicine -2005. -No. 3. - p.6-9. |
| [14] | Aranovich V.V., Svinarov M.Yu. Results of long-term follow-up observation of children living in an iodine-deficient region // Mater. IV AllRussiancongress of endocrinologists. - SPb. 2001. -p.576. |
| [15] | Autoimmune diseases of the thyroid gland / I.I. Delov. W.A. Groshina, S.S. Antonova et al. // Problems of endocrinology. -2002. -№2. - p.6-13. |
| [16] | Gerasimov G.A., Sviredenko N.Y. Iodine deficiency diseases. Diagnostics, methods of prevention and treatment // Therapeutics archive -1999 - No. 10. -p. 17-19. |
| [17] | Monitoring of iodine supply in pubertal schoolchildren in Mirninsky ulus of the Sakha Republic (Yakutia) / V.G. Selyatitskaya, N.A. Palchnikova, S.V. Odintsov et al. // Problems of endocrinology. - M., 2003. - No. 3. - p. 24-26. |
| [18] | Results of epidemiological studies of iodine deficiency diseases in the Russian Federation (IDD) in the framework of the “Tyromobile” project. Problems of biology and medicine. - 2005. - No. 3. - p. 19-20. |