Kholmurodova Adiba Shermamatovna
Department of Obstetrics and Gynecology FPDO Samarkand Medical Institute
Correspondence to: Kholmurodova Adiba Shermamatovna, Department of Obstetrics and Gynecology FPDO Samarkand Medical Institute.
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The cervix, due to its structural and functional features, occupies a special place in the reproductive system. Despite modern advances in the diagnosis and treatment of diseases of the cervix, its pathology continues to be the most important problem for both science and practical health care. The number of patients with cervical cancer under the age of 30 has more than doubled in recent years. In the structure of causes of death of women under 30 years of age, cervical cancer is 8.5% [3,5].
Keywords:
Reproductive system, Pathology, Cervical cancer
Cite this paper: Kholmurodova Adiba Shermamatovna, The Role of Molecular Genetic Polymorphisms in the Formation of the Progression of Cervical Intraepithelial Neoplasias, American Journal of Medicine and Medical Sciences, Vol. 12 No. 1, 2022, pp. 26-30. doi: 10.5923/j.ajmms.20221201.05.
1. Introduction
The high incidence of neoplastic processes in the cervix is explained by the increasing prevalence of human papillomavirus infection [1,4]. It is known that cervical intraepithelial neoplasias are stages of cervical carcinogenesis of three degrees: CIN I (mild dysplasia), CIN II (moderate dysplasia), CIN3 (severe dysplasia). At each stage, persistence, progression and regression are possible. According to the information center for the study of diseases caused by HPV, in the world as a result of screening in 2010, 300 million people infected with HPV of high and low carcinogenic risk and 10 million CIN3 were registered. With CIN 1, the probability of regression is high (60-70%) - only 11-20% of CIN 1 progresses to CIN II, and very rarely regressing CIN 2-3 are already an obligate precancer [2,5]. The molecular genetic mechanisms of persistence, regression, or progression to invasive cancer are not fully understood and understood. As the world practice shows, the results of treatment of cervical intraepithelial neoplasias, despite a wide variety of technologies and correction, are not very satisfactory. Also, the possibility of progression or regression of the development of pathology of the cervix after treatment of cervical intraepithelial neoplasias has not been studied. There is information about the progression of diseases of the cervix in connection with an underestimation of the degree of epithelial damage based on the material of limited biopsies, which led to improper patient management. The aim of this study was to determine the features and role of the polymorphic variant of the COL1A1 gene (C1997A) in women with cervical intraepithelial neoplasia of the cervix in the formation of CIN progression.
2. Material and Methods
To study the features and role of the polymorphic variant of the COL1A1 (C1997A) gene in 120 women with cervical intraepithelial neoplasia of the cervix, we assessed the distribution of the expected (Hexp) and observed (Hobs) frequencies of genotypic variants by polymorphism of the COL1A1 (C1997A) gene for compliance with Hardy's equilibrium -Wineberg (RHB, p> 0.05) in the group of patients with CIN of the cervix and among healthy women.
3. Results
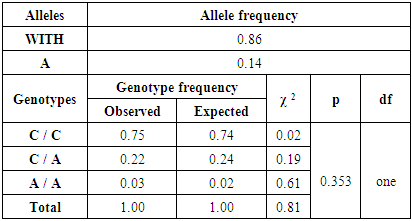
The observed frequencies of variants of the genotypes CC, C / A, and A / A in the generalized group of women with cervical CIN by polymorphism of the COL1A1 gene (C1997A) were 0.75, 0.22 and 0.03 and 0.52. Along with this, the shares of their expected frequencies were equal to 0.74, 0.24 and 0.02. The difference between the expected and observed frequencies of genotypes for the studied genetic polymorphism was not statistically significant (χ2 = 0.81; p = 0.353; df = 1), which confirms the absence of a discrepancy from RHV (table 1).Table 1. Expected and observed frequencies of distribution of genotypes of COL1A1 (C1997A) gene polymorphism by RHV in the main group of patients with cervical intraepithelial neoplasias
 |
| |
|
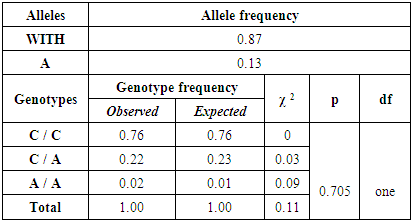
The absence of deviation from RHV was also observed in healthy women, among which the expected (Hexp) and observed (Hobs) frequencies of variants of the C / C, C / A and A / A genotypes for the COL1A1 gene polymorphism (C1997A) were 0.76 and 0, 76; 0.22 and 0.23; 0.02 and 0.01 (χ 2 = 0.11; p = 0.705; df = 1) (table 2). Table 2. Expected and observed frequencies of distribution of genotypes of COL1A1 (C1997A) gene polymorphism by RHB in the control group
 |
| |
|
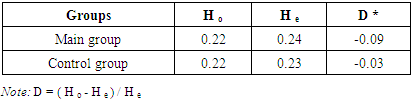
Analysis of the difference between the expected and observed frequencies of heterozygosity in the COL1A1 (C1997A) gene in the studied groups of patients with cervical CIN and healthy women showed its correspondence according to the results of the observed (Hobs) and expected (Hexp) genotype frequencies in the main group of women with CIN cervix 0.22 and 0.24 (D = -0.09), respectively, and among healthy people - 0.22 and 0.23 (D = -0.03), respectively (Table 3). Table 3. The difference between the expected and observed frequencies of heterozygosity in the COL1A1 gene (C1997A) in the studied main and control groups
 |
| |
|
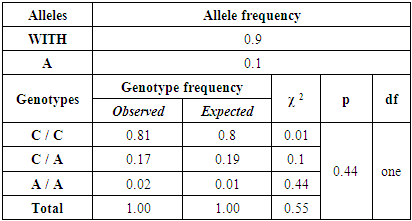
Consequently, from the above results, it is obvious that there are no statistically significant differences between the expected and observed proportions of genotypes in the main group of women with cervical CIN and healthy women according to the variant of the COL1A1 polymorphic gene (C1997A), which proves the absence of deviations in RHV.The further assessment of the distribution of the proportions of expected (Hexp) and observed (Hobs) genotypes C / C, C / A, and A / A by polymorphism of the COL1A1 gene among patients with CIN I showed their correspondence to the values 0.81 and 0.8 (χ2 = 0.01); 0.17 and 0.19 (χ2 = 0.1); 0.02 and 0.01 (χ2 = 0.44) with a statistically insignificant difference equal to p = 0.44 (table 4).Table 4. Expected and observed frequencies of distribution of genotypes in the COL1A1 (C1997A) gene by RHB among patients with CIN I
 |
| |
|
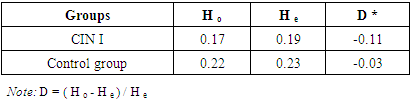
In the studied groups, the difference between the observed (Hobs) and expected (Hexp) proportions of genotypes for the COL1A1 gene polymorphism (C1997A) among patients with cervical CIN I was 0.17 and 0.19, respectively, with a heterozygosity index (D) corresponding to -0.11, and in healthy women - 0.22 and 0.23, respectively, with D = -0.03 (table 5).Table 5. The difference between the expected and observed frequencies of heterozygosity in the COL1A1 gene (C1997A) in the studied groups
 |
| |
|
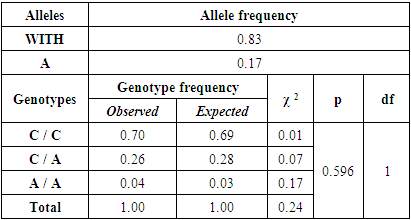
The shares of expected (Hexp) and observed (Hobs) genotypes C / C, C / A, and A / A for the COL1A1 gene polymorphism (C1997A) in the group of patients with CIN II were 0.70 and 0.69 (χ2 = 0.01); 0.26 and 0.28 (χ2 = 0.07); 0.04 and 0.03 (χ2 = 0.17), the difference between which was not significant (χ2 = 0.24; p = 0.596, df = 1) (Table 6).Table 6. Expected and observed frequencies of distribution of genotypes in the COL1A1 (C1997A) gene among patients with CIN II
 |
| |
|
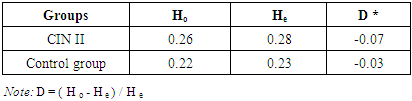
The difference between the observed (Hobs) and expected (Hexp) proportions of genotypes for COL1A1 (C1997A) gene polymorphism among patients with cervical CIN II was 0.26 and 0.28, respectively, with a heterozygosity index (D) corresponding to -0.07, and in healthy women - 0.22 and 0.23, respectively, with D = -0.03 (table 7).Table 7. The difference between the expected and observed frequencies of heterozygosity in the COL1A1 gene (C1997A) in the studied groups
 |
| |
|
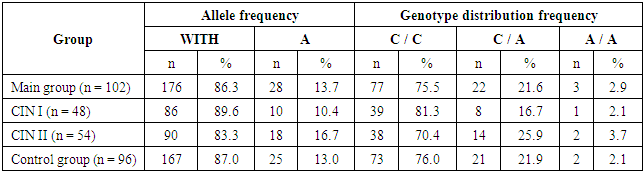
Thus, the analysis of the results of the distribution of observed and expected genotypic frequencies for the polymorphism of the COL1A1 (C1997A) gene in the generalized group of patients with CIN, as well as with CIN I and CIN II of the cervix, compared with those in healthy women, showed no deviation in RHV, that directly provides the opportunity to conduct subsequent stages of statistical research.In this regard, we studied the peculiarities of the occurrence of allelic and genotypic frequencies for the polymorphism of the COL1A1 (C1997A) gene in the combined group of women with CIN in comparison with those among the group of healthy women (Table 8).Table 8. Distribution of alleles and genotypes of COL1A1 (C1997A) gene polymorphism among patients with cervical intraepithelial neoplasia and in controls
 |
| |
|
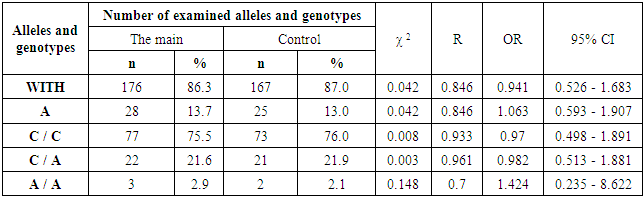
Thus, in the groups of women with CIN and healthy groups, allele C was detected in 86.3% and 87.0% of cases, and allele A in 13.7% and 13.0 cases, respectively. At the same time, a corresponding distribution was observed in relation to genotypic variants: in the group of patients with CIN, genotypes C / C, C / A, and A / A were detected in 75.5%, 21.6% and 2.9% of patients, respectively, and among healthy patients in 76.0%, 21.9% and 2.1% cases, respectively.Analyzing the distribution of alleles and genotypes by polymorphism of the COL1A1 (C1997A) gene among patients with CIN I and CIN II in comparison with the control, some peculiarities were traced. For example, in the group of women with CIN I, alleles C and A were detected in 89.6% and 10.4% of patients, and in the group of women with CIN II in 83.3% and 16.7% of cases (see Table 8). At the same time, variants of the C / C, C / A and A / A genotypes were observed in 81.3%, 16.7% and 2.1% of cases, respectively, among patients with CIN I and in 70.4%, 25.9% and 3.7% of cases, respectively, among patients with CIN II.The given values show the presence of differences in the proportion of the occurrence of alleles and genotypes of the polymorphic gene COL1A1 (C1997A) among the studied groups. To assess the significance of the revealed differences, we carried out a comparative analysis of them among women with CIN in comparison with the group of healthy women.Among the generalized group of women with CIN compared with healthy women, the differences in the frequency of alleles C (χ2 = 0.042; p = 0.0846; OR = 0.941; 95% CI: 0.526 - 1.683) and A (χ2 = 0.042; p = 0.846; OR = 1.063; 95% CI: 0.593 - 1.907) did not differ in statistical significance. Similarly, the absence of significant differences was also revealed for the variants of the C / C genotypes (χ2 = 0.008; p = 0.933; OR = 0.97; 95% CI: 0.498 - 1.891), C / A (χ2 = 0.003; p = 0.961; OR = 0.982; 95% CI: 0.513 - 1.881) and А / А (χ2 = 0.418; p = 0.7; ОR = 1.424; 95% CI: 0.235 - 8.622) (Table 9). Table 9. Differences in the distribution of allele frequencies and genotypes of COL1A1 (C1997A) gene polymorphism among patients with cervical intraepithelial neoplasias and in the control group
 |
| |
|
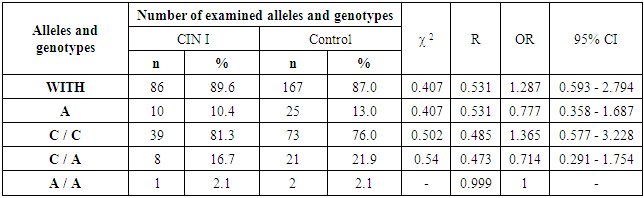
Analysis of the distribution of allele variants and genotypes by COL1A1 (C1997A) gene polymorphism in comparison with the healthy group among women with CIN I also showed no significant differences in the distribution of C allele frequencies (χ2 = 0.407; p = 0.531; OR = 1.2879; 95% CI : 0.593 - 2.794) and А (χ2 = 0.407; p = 0.531; ОR = 0.777; 95% CI: 0.358 - 1.687) and genotypes С / С (χ2 = 0.502; p = 0.485; ОR = 1.365; 95% CI: 00.577 - 3.228), С / А (χ2 = 0.54; p = 0.473; ОR = 0.714; 95% CI: 0.291 - 1.754). The proportion of the frequency of the mutant genotype A / A was practically equal in both groups (2.1% versus 2.1%) (Table 10). Table 10. Difference in the frequency distribution of alleles and genotypes of COL1A1 (C1997A) gene polymorphism among patients with CIN I and in the control group
 |
| |
|
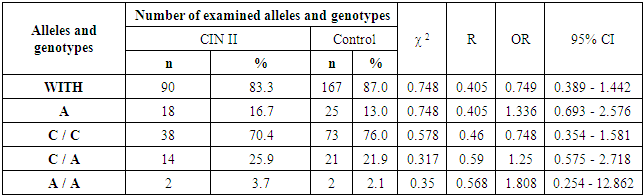
Thus, a comparative analysis in the group of women with CIN I compared with the control group showed differences of more than 1.2 and 1.3 times only in relation to the favorable C allele (89.6% versus 87.0%) and the C / C genotype (81.3% versus 76.0%) ... However, they, like the remaining allele and genotypes, did not have statistical significance. In this regard, it can be concluded that allelic and genotypic variants for the COL1A1 gene polymorphism (C1997A) do not independently affect the mechanisms of CIN I formation.An analysis of comparison in the distribution of allele variants and genotypes of COL1A1 (C1997A) gene polymorphism among women with CIN II compared with healthy women also revealed a lack of reliability in the proportion of C allele frequencies (χ2 = 0.748; p = 0.405; OR = 0.749; 95% CI: 0.389 - 1.442) and А (χ2 = 0.748; p = 0.405; ОR = 1.336; 95% CI: 0.693 - 2.576), and, at the same time, in the fractions of frequencies of genotypes С / С (χ2 = 0.578; p = 0.46; ОR = 0.748; 95% CI: 0.354 - 1.581), С / А (χ2 = 0.317; p = 0.59; ОR = 1.25; 95% CI: 0.575 - 2.71882) and А / А (χ2 = 0.35; p = 0.568; ОR = 1.808; 95% CI: 0.254 - 12.862) (Table 11). Table 11. Difference in the distribution of allele frequencies and genotypes of COL1A1 (C1997A) gene polymorphism among CIN II patients and in the control group
 |
| |
|
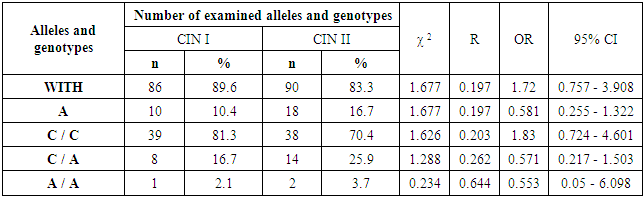
According to these data, it can be seen that in the group of women with CIN II, according to the polymorphism of the COL1A1 (C1997A) gene, compared with healthy women, there is an increase in the frequencies of unfavorable allele A by more than 1.3 times (16.7% versus 13.0%), genotypes C / A by 1.25 times (25.9% versus 21.9%) and A / A 1.81 times (3.7% versus 2.1%). However, these differences also turned out to be statistically not significant, which allows us to conclude that there is no independent role for the COL1A1 (C1997A) gene in the development of CIN II.Meanwhile, we found it very interesting to study the differences between the groups of women with CIN I and CIN II. In this regard, we found important facts characterized by tracing a tendency towards a decrease in the favorable allele C by a factor of 1.72 (89.6% versus 83.3%; χ2 = 1.677; p = 0.197; OR = 1.72; 95% CI: 0.757 - 3.908) and genotype C / С by 1.83 times (81.3% versus 70.4%; χ2 = 1.626; p = 0.203; OR = 1.83; 95% CI: 0.724 - 4.601) among women with CIN II. Moreover, in the group of women with CIN II, a tendency to an increase in the frequency of unfavorable heterozygous genotype C / A was registered (16.7% versus 25.9%; χ2 = 1.288; p = 0.262; OR = 0.571; 95% CI: 0.217 - 1.503) (table 12).Table 12. Difference in the frequency distribution of alleles and genotypes of COL1A1 (C1997A) gene polymorphism in patients with CIN I and CIN II
 |
| |
|
Consequently, the revealed high frequencies of the C allele and the C / C genotype among women with CIN I indicate their protective activity against the transition to CIN II, and, conversely, a large proportion of carriers of the unfavorable C / A genotype among women with CIN II shows a tendency to increase risk of developing this form of CIN.
4. Conclusions
1. Studies to study the features of the COL1A1 (C1997A) gene polymorphism both in the general group of women with CIN and in groups with CIN I and CIN II confirm the absence of statistically significant differences in the carriage of allelic and genotypic variants of this gene. 2. The found differences in the frequency of the C allele and the C / C genotype between the groups of women with CIN I and CIN II show a tendency towards their protective role in the formation of CIN II, while in relation to the unfavorable C / A genotype, a tendency to an increased risk of CIN II formation was observed.
References
| [1] | Apolikhina I.A., Baryshnikov A. Yu. Papillomavirus infection of the genitals: an urgent problem of modern gynecology and ways to solve it / I.A. Apolikhina, E. D. Denisova // Vopr. gynecology, obstetrics and perinatology. - 2007. - T. 6, No. 6. - S. 70-75. |
| [2] | Kiselev and V.I. The etiological role of the human papillomavirus in the development of cervical cancer: genetic and pathogenetic mechanisms I.O. Kiselev, // Cytokines and inflammation. - 2003. - T. 2, No. 4. P.31-38. |
| [3] | Podistov, Yu.I. Epithelial dysplasia of the cervix (diagnosis and treatment) / Yu.I. Podistov, K.P. Laktinov, N.N. Petrovichev, V.V. Bryuzgin. - M.: Geotar-Media, 2006. -- 138 p. |
| [4] | Brusselaers, N., Shrestha, S., Van De Wijgert, J., & Verstraelen, H. (2018). Vaginal dysbiosis, and the risk of human papillomavirus and cervical cancer: systematic review and meta-analysis. American Journal of Obstetrics and Gynecology. doi: 10.1016/j.ajog.2018.12.011. |
| [5] | Liman Yang1, Jing Jin1, Juhong Liu // Correlation of MMP2-C1306T (rs243865) and MMP7-181A / G (rs11568818) with cervical cancer: a meta-analysis. European Journal of Gynaecological Oncology 2020, Vol. 41 Issue (4): 508-512. |
| [6] | Seliakova MS, Ageeva TA, Savchenko SV Relationship between metalloproteinase and TIMP1 expression and intensity of cervical inflammatory reaction in women of different age groups with cervical intraepithelial neoplasia and microinvasive carcinoma // Siberian Journal of Oncology. 2019; 18 (6): 50–56. - doi: 10.21294/1814-4861-2019-18-6-50-56. |
| [7] | Shuchi Shukla, Sabuhi Qureshi, Uma Singh, and Sanjay Khattri. A Study of Matrix Metalloproteinase-2 and Interleukin-18 in Preinvasive and Invasive Lesions of Cancer Cervix // J Midlife Health. 2020 Oct-Dec; 11 (4): 236-239. |
| [8] | Akhmatova G.R.The formation of spiritual education is one of the priorities in human life and society. European Journal of Research and Reflection in Educational Science .Vol.7, №12, 2019. ISSN 2056-5852\498-500 P. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML