-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(12): 891-895
doi:10.5923/j.ajmms.20211112.10
Received: Dec. 2, 2021; Accepted: Dec. 19, 2021; Published: Dec. 20, 2021

Endoscopic Technologies in Diagnostics and Treatment of Acute Epididymo-orchitis and Other Diseases Leading to Acute Scrotum Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLT. M. Berdibaev , A. K. Kuchkarov
Center for the Development of Professional Skills of Medical Staff under the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article provides information on the diagnosis and treatment of several diseases associated with acute scrotal syndrome. Also, in this article, the authors use endoscopic diagnosis and treatment of acute epididymitis and provide data from their own observations. An acute scrotum is a condition characterized by pain, swelling, and redness of the skin in the corresponding area of the scrotum. The diseases leading to this syndrome can be varied, as well as the tactics of their treatment. From January 2017 to May 2021, 214 patients with a diagnosis of acute nonspecific epididymitis or epididymo-orchitis were treated in the urology department of the 1-City Clinical Hospital named after Ibn-Sino in Tashkent. 151 (70.5%) of them received outpatient treatment before hospitalization, which did not improve their condition. 207 out of 214 patients underwent surgical treatment. The average length of hospital stays in patients who underwent surgery - traditional epididymotomy - was longer than in those operated on minimally invasive way. Assessment of pain on a 10-point scale showed that patients undergoing minimally invasive surgery experienced less pain in the immediate postoperative period than patients who underwent traditional epididymotomy.
Keywords: Epididymo-orchitis, Epididymitis, Orchitis, Torsion of the spermatic cord, Morgagni's hydatid, Acute scrotum, Diagnosis, Treatment, Scrotoscopy
Cite this paper: T. M. Berdibaev , A. K. Kuchkarov , Endoscopic Technologies in Diagnostics and Treatment of Acute Epididymo-orchitis and Other Diseases Leading to Acute Scrotum Syndrome, American Journal of Medicine and Medical Sciences, Vol. 11 No. 12, 2021, pp. 891-895. doi: 10.5923/j.ajmms.20211112.10.
1. Introduction
- An acute scrotum is a condition characterized by pain, swelling, and redness of the skin in the corresponding area of the scrotum.The diseases leading to this syndrome can be varied, as well as the tactics of their treatment.The causes of pain, hyperemia and edema in the scrotum can be the following diseases: 1. Infectious diseases such as acute epididymitis, orchitis, scrotal abscess, gangrenous infections of the scrotum. 2. Ischemic diseases such as torsion of the spermatic cord, torsion of the testis or epididymis. 3. Injury to the scrotum. 4. Irreducible, restrained groin-scrotal hernia. 5. Other diseases such as hemorrhagic vasculitis, scrotal vasculitis; acute leukemic testicular infiltration. 6. Acute conditions in chronic pathology: rupture or bleeding with spermatocele; infection, rupture or bleeding with dropsy of the testicle, etc. [1]Acute epididymo-orchitis is an inflammation of the testicle and its epididymis manifested by pain, swelling, reddening of the scrotum and fever. Epididymitis is an isolated inflammation of the epididymis [1,2]. Isolated orchitis is much less common, most often with the hematogenous pathway of infection. The spread of the inflammatory process to the testicle with the development of acute epididymo-orchitis is observed, according to various authors, in 10-58% of cases [3,4]. Chronic epididymitis refers to epididymal pain and inflammation, usually without scrotal edema, that lasts more than six months [5]. The disease is predominantly unilateral, a bilateral process is observed in 5-10% of patients and is more common in tuberculous epididymitis [6,7].In acute epididymitis, inflammation of the epididymis occurs mainly due to nonspecific and specific infectious genesis, but it can also develop as a result of viral infections, trauma, autoimmune disorders, medication (amiodarone), etc. [8]. Most often, infection occurs through the canalicular route and is a complication of urethritis, prostatitis, cystitis. With the canalicular pathway of infection, the inflammatory process first of all develops in the tail of the epididymis, then passes into the body, the head of the epididymis, and subsequently passes into the testicle.Pain and swelling are common symptoms of acute epididymitis. The edema usually begins in the tail of the epididymis before it rises to involve the entire epididymis and finally reaches the testicle.The clinical picture of acute epididymitis ranges from mild epididymal tenderness to severe, febrile systemic disease, including urosepsis [9].Before the onset of symptoms of acute epididymitis, signs of prostatitis, urethritis may precede, and you should also ask about sexually transmitted history and endoscopic examinations in the urinary tract.On an objective examination, there may be signs of intoxication such as fever and tachycardia. Local palpation symptoms such as a thickened spermatic cord, the appendage is indurated and edematous, Fern’s sign is positive (if the testicle is raised, the pain decreases), the Cremaster reflex is present in the early stages of epididymitis. [10,11].Standard diagnostics for acute epididymitis include:• Ultrasound examination, which reveals hypo echogenicity and an increase in the epididymis, an increase in blood flow to it, an inflammatory infiltrate or abscess.• MRI gives more accurate information about the condition of the testicle and its epididymis, but due to the high cost and lack of this method in ordinary urological clinics, it is not widely used.To identify the pathogen, urine culture is performed, a smear from the urethra is examined, and if suspected, it is examined for tuberculosis. It is important to take a complex examination to exclude other urological pathology.The treatment consists of general principles such as: rest, exalted position, pain relievers. Antibiotic therapy is carried out against the alleged pathogen. Surgical treatment is carried out when conservative treatment is ineffective or when purulent foci are identified using an ultrasound examination. Traditionally, surgery involves revision of the testicle and epididymis. When local purulent foci of the epididymis are detected, the foci are opened, an epididymotomy or resection of the epididymis is performed. With a total purulent lesion of the epididymis, it is removed.Testicular torsion is most common in children and adolescents, but this diagnosis should be considered when evaluating patients with scrotal pain of any age. In the mechanism of development of torsion of the spermatic cord, the leading role is played by a sharp contraction of the cremaster muscle, the fibers of which have a spiral course. This causes the testicle to rotate as it is pulled up to the outer groin ring. During torsion of the spermatic cord, the veins of the spermatic cord are first compressed, with further rotation, the arteries are compressed with the development of ischemia and infarction of the testicular tissue.Torsion of the spermatic cord can be intravaginal, which occurs in the cavity of its own vaginal membrane and is a consequence of the lack of connection along the posterior surface of the testicle and the tunicae vaginalis.It can be extravaginal when torsion occurs outside the cavity of the own vaginal membrane. Torsion can occur between the epididymis and the testicle.When the spermatic cord is twisted, the pain begins sharply, radiating to the groin area, the lower abdomen. Sometimes the pain is accompanied by vomiting and a collaptoid condition.During an objective examination of patients with torsion of the spermatic cord, palpation determines the soreness of the gonads, its increase, tightness to the root of the scrotum or to the external inguinal ring. A twisted testicle is inactive, raised, its longitudinal axis can be displaced. When you try to raise the testicle even higher, the pain intensifies. There is no cremasteric reflex. The onset of the pain symptom may be preceded by trauma, physical activity, however, cases of torsion of the spermatic cord and at rest (for example, during sleep) have been described.An ultrasound examination at the onset of the disease shows a normal picture. During a period of 4-6 hours, the testes are usually edematous and hypoechoic, after 24 hours they have a heterogeneous structure, which is associated with vascular obstruction, hemorrhage and necrosis. Doppler sonography is important, which detects the complete absence of blood flow or its decrease. However, the preservation of arterial blood flow does not exclude this diagnosis (in 24% of cases in boys with testicular torsion, the blood supply to the latter was normal or increased) [1].Treatment is usually surgical. If the testicle is viable, then the testicle is fixed (orchiopexy) with separate sutures for the vaginal or dartosis. When the surgery is performed at a later date and the testicle is not viable, orchiectomy is performed. In the presence of a wide vaginal cavity (bell-tongue symptom) during an operation for testicular torsion, it is advisable to perform orchipexy of the contralateral testicle.Morgagni's gidatids are also prone to twisting, as they hang on thin legs.Torsion of hydatids is manifested by sudden pain of varying intensity, arising in the scrotum, iliac or groin region, then shifting to the testicle.On objective examination, testicular mobility and cremasteric reflex are preserved. The vertical orientation of the longitudinal axis of the testicles is preserved. In the early stages of the disease, gidatid often appears through the skin of the scrotum in the form of a dark blue knot, sometimes a painful seal can be palpated at one of the poles of the testicle. The testicle itself is painless on palpation. Later, there is edema, enlargement and redness of the scrotum.On Doppler ultrasound, hydatid torsion does not have an internal blood flow signal, while increased vascularization may be observed around it. When the diagnosis of hydatid torsion is beyond doubt, analgesics can be treated.The main distinguishing features of these conditions:In acute epididymitis, the pain is moderate, the symptoms are present for several days, it can occur in all age groups, at first the tail of the epididymis swells, then the entire epididymis and the testicle itself, the testicle position is normal, the pain decreases when the testicles are raised, there are signs of inflammation, leukocytosis, pyuria, fever. Doppler ultrasonography increases blood flow.With torsion of the spermatic cord: The pain is severe, the duration of the symptoms is several hours, it occurs mainly in children and adolescents, the position of the testicles is elevated, transverse, with Doppler ultrasound, blood flow is absent or reduced.Torsion of Morgagni's hydatids occurs in children. The pain is usually mild and begins gradually. One can observe swelling in the region of the epididymis head, sometimes it is possible to palpate the node [12,13,14].Everything seems to be easy, simple and understandable. But there are cases that a teenager with acute pain in the lower abdomen turns to the surgeon, who excludes appendicitis, prescribes analgesics and antispasmodics. And a day later, his pain passes into the scrotum. On examination, she is already hyperemic, edematous, ultrasound gives a picture of epididymitis, and then for a couple of days he is being treated for epididymitis. At the end, during the audit, it is revealed that the patient has a torsion of the spermatic cord. Or in a patient with acute epididymitis, symptoms lasting 5-6 days, an ultrasound scan is performed and no purulent foci are found, which would serve as an indication for surgery. The patient is treated conservatively for a long time, but without effect. Since the information content of ultrasound diagnostics is often associated with the qualifications and experience of the diagnostician.Our observations show that a fairly large number of patients with acute nonspecific epididymitis treated with standard conservative therapy in the future required surgical treatment due to the ineffectiveness of therapy.This was the reason for conducting research, the purpose of which is to improve the diagnosis and treatment of patients with acute nonspecific epididymitis using endoscopic technologies.The purpose is to study: Introduce into the clinic the technique of endovideo diagnosis of acute epididymitis and assess the diagnostic value of this method; To develop and introduce into practice a minimally invasive endoscopic method for the treatment of acute epididymitis and to study the results of this method.To achieve the goals and objectives, a method has been developed - Scrotoscopy and epididymotomy using a holmium laser.
2. Materials and Methods
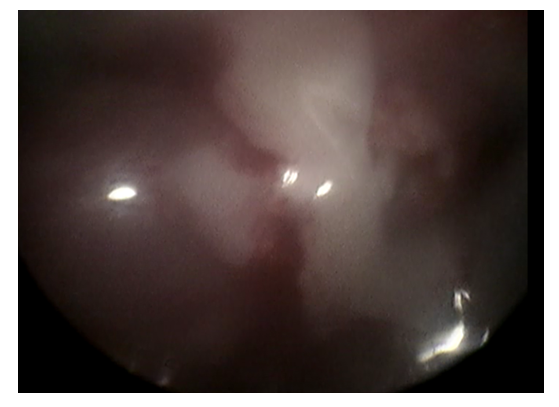
- From January 2017 to May 2021, 214 patients with a diagnosis of acute nonspecific epididymitis or epididymo-orchitis were treated in the urology department of the 1-City Clinical Hospital named after Ibn-Sino in Tashkent. 151 (70.5%) of them received outpatient treatment before hospitalization, which did not improve their condition. 207 out of 214 patients underwent surgical treatment, of which:• 157 (75.84%) - epididimotomy, which means that incisions were made on the fascial membrane of the epididymis and / or purulent foci were drained.• 10 (4.83%) patients had epididymectomy - the appendage was removed.• 16 (7.72%) - patients with epididymoectomy - removed the testicle and epididymis together.• 24 (11.59%) patients underwent scrotoscopy. Which ended• In 16 (66.66%) patients - laser epididimotomy.• In 5 (20.88%) - patients with open epididymotomy due to a pronounced adhesive process between the epididymis and the vaginal membrane.• In 1 (4.16%) patient, open orchiepididymectomy.• In 2 x (8.33%) - open epididymectomy for torsion of the spermatic cord.Premedication is carried out 30 minutes before the operation, preferably with an intramuscular narcotic analgesic. The operation is performed in the operating room, in a horizontal position of the patient on the operating table. The operating field is treated with an antiseptic solution. Local anesthesia: Lorin-Epstein blockade is performed by injecting 50-60 ml -0.5% Novocain solution into the spermatic cord, then local infiltrative Novocain anesthesia is performed. An incision of the skin of the scrotum with a length of 10-12 mm is performed, parallel to the Rafé line, laterally. The muscular membrane is opened in a blunt and sharp way, hemostasis is performed as needed. After visualization of the vaginal membrane, the latter is opened and held on soft clamps or handles on sutures are applied. A 14Fr children's cystoscope is inserted into the cavity of the vaginal membrane (you can use a mini nephroscope, ureterorenoscope) to which a system with a supply of warm saline is attached to irrigate the cavity of the vaginal membrane and to improve visualization. The attached camera on the cystoscope displays an enlarged image on the monitor screen. Visualization of the testicle and its epididymis is performed, the purpose of which is to examine the condition of the testicle and its epididymis, for the presence of edema, redness, apostems and / or abscesses. (Photo 1, 2).
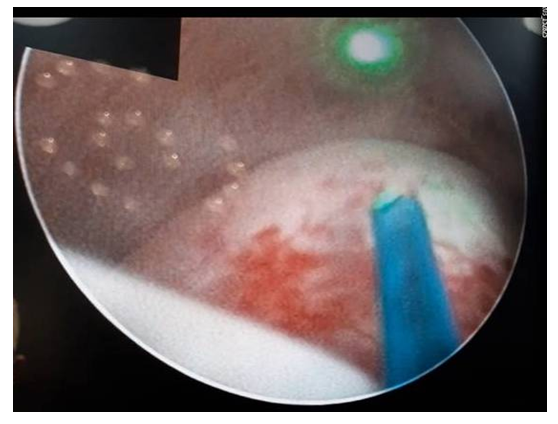 | Photo 1. Inflamed, hyperemic appendage, covered with fibrinous plaque |
 | Photo 2. Forming abscess from several apostems |
 | Photo 3. Decompression of the epididymis abscess |
3. Results and Discussion
- Before the operation, according to ultrasound data, purulent foci were detected in 8 (3.86%) patients out of 207 operated, and during revision purulent foci were detected in 162 (78.26%) patients, respectively.The average length of hospital stay in patients who underwent surgery - traditional epididymotomy - was longer than in those operated on minimally invasive way. Assessment of pain on a 10-point scale showed that patients operated on minimally invasive experienced less pain in the immediate postoperative period than patients who underwent traditional epididymotomy (Table 1).
|

4. Conclusions
- Patients with acute epididymo-orchitis are subject to inpatient treatment and active observation in a urological hospital.The method of scrotoscopy and laser epididimotomy with the use of a holmium laser allows visualizing the condition of the testicle and its epididymis in acute diseases of the scrotum, identifying foci of purulent inflammation and simultaneously draining them in a minimally invasive way in acute epididymitis. Significantly increase the information content of the diagnosis of acute epididymitis and other conditions of the acute scrotum syndrome, improve the results of its treatment in a minimally invasive way, shorten the days of hospital stay, and achieve early activation and rehabilitation of the patient.