-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(11): 765-768
doi:10.5923/j.ajmms.20211111.04
Received: Oct. 17, 2021; Accepted: Oct. 30, 2021; Published: Nov. 15, 2021

The NIPS Scale as an Alternative Method of Assessing Myofascial Pain in Children with Obstetric Paralysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdusalomova M. A., Ravshanova M. A., Burxanova G. L., Ismoilov J. K.
Samarkand State Medical Institute, Samarkand, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article scales myofascial pain in children with obstetric paralysis (NIPS and FLACC). However, the effectiveness of kinesiological tapes in the treatment of myofascial pain has been reported. Research materials and methods. 45 sick children of different stages of the disease were examined (main group). The control group consisted of 30 patients with no focal neurological signs. During the follow-up, all patients in the main group were divided into 2 subgroups: 27 children (60%) were included in subgroup 1, who received electrostimulation of the affected shoulder girdle, shoulder, wrist and palm muscles and kinesiological tapes in this area during the entire period of hospitalization. 18 (40%) children were included in the 2nd small comparison group, who were prescribed standard treatment for obstetric paralysis. Results and their discussion Although a positive result was observed in the comparative subgroup , it was found to be lower than in the main subgroup. In the main subgroup, the use of electrostimulation of the shoulder girdle, shoulder, wrist and palm muscles in combination with standard treatment allows to achieve effective results at the expense of cessation of demyelination processes, reduction of myofascial pain and quality regeneration. An increase in the amplitude of the M-response was observed after treatment in this group of patients.
Keywords: Children, Obstetric paralysis, Scale, Myofascial pain, Kinesiological tap, Rehabilitation
Cite this paper: Abdusalomova M. A., Ravshanova M. A., Burxanova G. L., Ismoilov J. K., The NIPS Scale as an Alternative Method of Assessing Myofascial Pain in Children with Obstetric Paralysis, American Journal of Medicine and Medical Sciences, Vol. 11 No. 11, 2021, pp. 765-768. doi: 10.5923/j.ajmms.20211111.04.
Article Outline
1. Relevance of the Study
- The urgency of the problem of birth injuries of the nervous system Despite the progress made in the course of the birth process, the incidence of this pathology remains high. Perinatal mortality is 11%. Congenital injuries in the neck area accounted for 86.5%. This is because even during a normal birth, the main load falls on this part of the spine. Currently, according to statistics, birth injuries account for 1% of all perinatal injuries. The detection of myofascial pain syndrome in 68% of these patients indicates the urgency of the problem. For a long time, the sensation of pain in newborns was not taken seriously by neonatologists. Newborns were considered to have no neurological basis for pain perception and were less sensitive to it. At the same time, there were opinions that the sensation of pain conducted does not lead to any negative complications and that analgesics in newborns cannot be recommended due to the high incidence of side effects. So far, many studies have shown that the nootropic system at birth showed anatomical and functional readiness to accept pain, even in premature infants. The aim of the study was to assess the degree of myofascial pain syndrome in patients with obstetric paralysis using scales and to compare the effectiveness of complex rehabilitation measures.
2. Materials and Research Methods
- Research and clinical observations were performed in 45 patients in the acute phase of the disease. 30 healthy children were taken as a control group. In the main group, boys - 20 (44.4%), girls - 25 (55.6%). The age of children is from 1 month to 3 years (average age). No anamnesis of focal neurological symptoms and movement disorders were observed in children in the control group. In the main group of patients, BMN focal pathologies, cervical symptoms, areflexia, hyporeflexia, and movement disorders were identified during the examination. Myofascial pain levels were assessed using NIPS (in patients under 1 year of age) and FLACC behavior scales (in patients under 3 years of age). The children's parents agreed to the investigation.
3. Results and Their Discussion
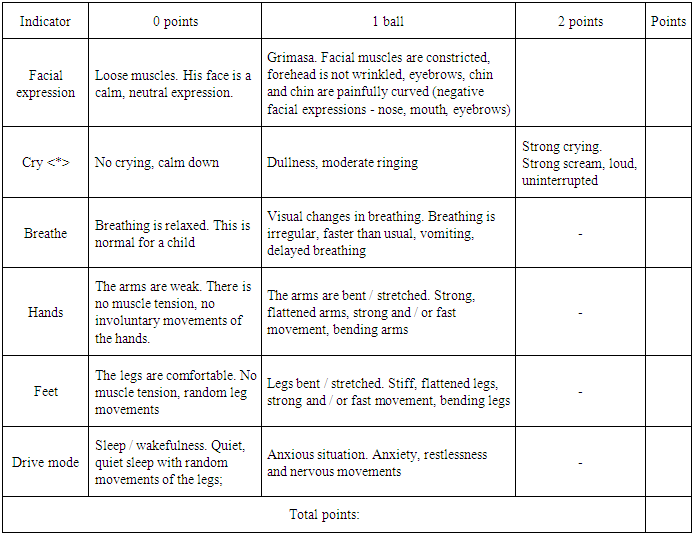
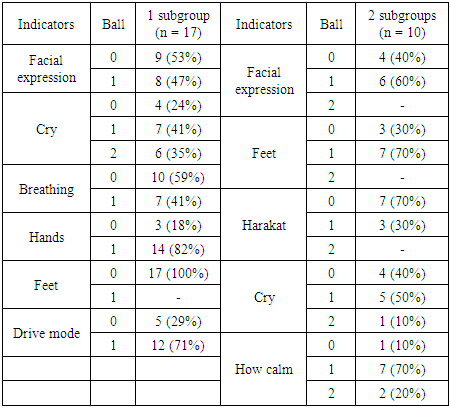
- After a neurological examination, the patients were diagnosed and complications of the disease were identified. During the follow-up, all sick children in the main group were divided into two subgroups: 27 children (60%) in group 1, who received electrostimulation and kinesiological tapes on the affected side during the entire hospitalization in addition to the main treatment. Children in subgroup 2 received standard treatment for 18 (40%) obstetric paralysis. In this study, patients with high, low, and total types of obstetric paralysis were taken. The upper type was attached to the affected shoulder joint area by pulling the shoulder girdle and the healing zone of the tap, while the spinal muscles were also taped with Y tapes from taps of various manufacturers (Kinesio tex gold, kinesiology tape). The palmar muscles were also corrected with lymphatics (weighing up to 50%). In patients with subtype paralysis, I taps were placed on the wrist muscles. In the area of the shoulder muscles, the Y taps were functionally corrected. In total type patients, taps were placed with 25-40% pull on the shoulder and wrist muscles. The tapes were replaced with new ones every 3 days. Pain levels were assessed at the time of the first examination, then on days 3 and 6. Patients in the main group were electromyostimulated with a current of 20-40 mA for 15-20 minutes during hospitalization.The degree of myofascial pain was assessed using the scales described below. A correlation of the diagnostic significance of both scales in assessing the rehabilitation potential of patients was then performed.The NIPS scale was used to assess myofascial pain levels in patients under 1 year of age. It consists of the following indicators: facial expression, crying, breathing, hands, feet, state of arousal. The pain level was expressed as the sum of the scores on all 6 indicators. 0 points - the minimum amount of the sum of points, 7 - the maximum maximum score. If the sum of the scores is higher than 3, it means pain (Lawrence et al., 1993). We used the FLACC scale to assess pain for sick children aged 1–3 years. It collected data on 6 indicators1. Face- Unclear facial expression or smile-0 points- Sometimes-grimasa or sliding eyebrows-1 point- Frequent or constant jaw tremors. Jaw tension-2 points2. Feet - normal condition, looseness-0 points- Can't find a normal position, always moves his legs. Legs tense.-1 point- lifting or kicking-2 points3. Movement- lips quietly, position is normal, moves slightly-0 points- turns, moves back and forth, stretched-1 point- bends like a bow; rigidity; siltash-2 points4. Cry- no crying (both while awake and asleep) -0 points- sighs or whispers; complains from time to time-1ball- Long cries, shouts or cries, often complains-2 points5. How calm you can be- satisfied, calm- 0 points- Soothes from touching, hugging, talking. Can be distracted-1 point- Difficult to calm down-2 pointsThe minimum score is 0, the maximum is 10 points. The higher the score, the stronger the pain and the worse the child feels.
|
|
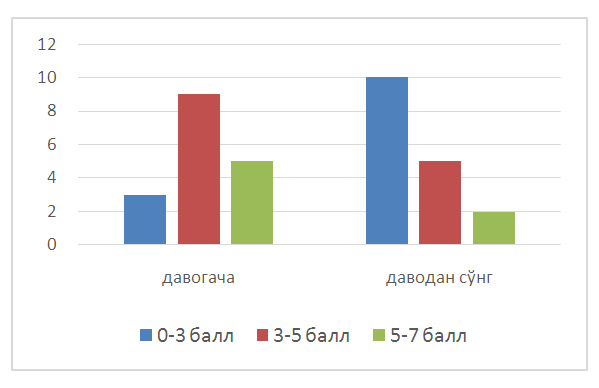 | Figure 1. Dynamics of myofascial pain in the main group on the NIPS scale |
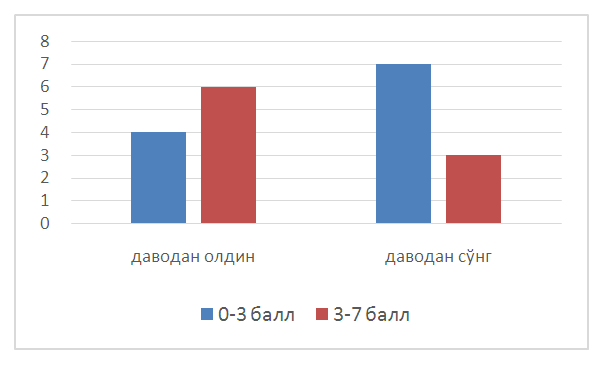 | Figure 2. Dynamics of myofascial pain in the main group on the FLACC scale |
4. Conclusions
- From the above, it can be concluded that although positive dynamics was observed in the comparative group, but less than in the main group. These data confirm the need to apply the above-listed rehabilitation measures in the early stages, ie in the absence of signs of demyelination. Our study showed that the use of electromyostimulation in combination with standard therapy allowed to stop demyelination processes in the main group and achieve many effective results at the expense of quality regeneration. In this group of patients, our data showed a 12% increase in M-response. There were no side effects during treatment.