-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(10): 725-728
doi:10.5923/j.ajmms.20211110.13
Received: Oct. 7, 2021; Accepted: Oct. 25, 2021; Published: Oct. 30, 2021

Application of Modern Technologies in the Treatment of Fractures and Dislocation of the Clavicle
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEsandavlat Mengziyevich Shukurov, Aziz Pulatovich Alimov, Anvar Akhtamovich Zhabbarov, Orif Negmatzhonovich Akhmadzhonov
Republican Specialized Scientific and Practical Center for Traumatology and Orthopedics Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Conclusion: Results of treatment were studied in 216 patients in adult's department, 89 patients of them had intramedullary osteosynthesis with spokes, 44 patients with acromial clavicle fractures had lavaloplasty and fixation with spokes, 83 patients had osteosynthesis with AO (LCP) plate given the character of fracture.
Keywords: Clavicle, Middle third, Fractures, Osteosynthesis, Bench tests, Preclinical studies, Intramedullary nail, Plate
Cite this paper: Esandavlat Mengziyevich Shukurov, Aziz Pulatovich Alimov, Anvar Akhtamovich Zhabbarov, Orif Negmatzhonovich Akhmadzhonov, Application of Modern Technologies in the Treatment of Fractures and Dislocation of the Clavicle, American Journal of Medicine and Medical Sciences, Vol. 11 No. 10, 2021, pp. 725-728. doi: 10.5923/j.ajmms.20211110.13.
Article Outline
1. Introduction
- Clavicle fractures account for 3 to 19% of all fractures and dislocations of the bones of the skeleton [1,7,9]. The relevance of this kind of damage is determined by the fact that they, as a rule, become the lot of young and middle-aged people leading an active and socially useful lifestyle [2,3,4]. The method of choice in the treatment of displaced, comminuted and unstable clavicle fractures is open reduction and osteosynthesis with nails or plates of various modifications. The incidence of unsatisfactory outcomes in submerged osteosynthesis of the clavicle is 25–30% [1,6] In recent years, the number of purulent complications in the surgical treatment of closed fractures has increased, which is associated with the expansion of indications for osteosynthesis of the limbs. The main part of these errors (60.3%) depends on the incorrect selection of metal structures, violations of the principles of asepsis, operational and technical errors during the operation, non-observance of the principles of correct postoperative immobilization of the limb. There is still a high incidence of unsatisfactory treatment results (42–50%) and recurrences of bone tissue inflammation (22–74.3%) [5,7,8]. a number of surgical methods of osteosynthesis have been proposed: 1) external transosseous; 2) submersible (includes intraosseous, extraosseous and transosseous). The emergence of new high-tech implants and osteosynthesis techniques, the increased requirements of patients for the quality of life, their early return to work, including even during the treatment of a fracture.The aim of the work was to improve the results of treatment of patients with clavicle fractures using modern surgical methods of treatment.
2. Materials and Methods
- Our study is based on the experience of surgical treatment of 216 patients with fractures and fracture-dislocations of the clavicle from 2018 to 2021. The patients' age ranged from 18 to 60 years. There were 156 men and 60 women. Patients were admitted to the clinic at various times after the injury. In the overwhelming majority of cases (98%), osteosynthesis of the clavicle was performed on the second and third day of admission to the hospital.
3. The Main Results and Findings
- All patients underwent treatment according to the developed algorithm for the diagnosis and choice of treatment tactics for the fracture of the acromial end of the clavicle (DGU 06556 dated 05/30/19). Clinical, X-ray and MSCT, ultrasound (vascular Doppler) study were used in the work. For a comparative assessment and more accurate differentiation in case of damage to the acromial end of the clavicle of the CAS, it was necessary to perform radiographs of both clavicular-acromial joints in the anteroposterior projection on the same film.When choosing the type of anesthetic treatment, preference was given to regional anesthesia. Brachial plexus blockade was performed with 0.5% bupicaine under ultrasound control with sedation in patients with upper limb injuries, which provided adequate and safe anesthesia, prolonged postoperative analgesia up to 12-15 hours.The choice of treatment and implant tactics was determined by the nature and location of the fractures. Three surgical options have been used to treat clavicle shaft fractures: We used AO plates (Bombei India), with a straight (DCP) and a pre-curved (anterior-superior) plate (LCP) with locking.The 1st group consisted of 89 patients who underwent surgery intramedular osteosynthesis with wires,Group 2 - 44 patients in whom lavsanoplasty and fixation with wires were performed with fracture dislocations of the acromial end of the clavicle.Group 3 consisted of 83 patients who underwent external osteosynthesis with an AO plate (Arbeitsgemeinschaft fur Osteosynthesefragen).In order to illustrate the efficiency of bone osteosynthesis in the treatment of clavicle fractures, we present the following clinical observations.Extra bone osteosynthesisa) Reconstructive simulated plate 2.0; 3.5 mm thick for osteosynthesis of fractures, (LCP Bombei India).Reconstructive plates had advantages, depending on the configuration of the clavicle, allowing them to be installed in fractures, in almost any location.Osteosynthesis of the clavicle was carried out in 3 stages - first, the plate on the clavicle is modeled according to the curvature of the bone, then the model is applied to its surface (from above or in front) and fixed with screws to the bone fragments; In case of a fracture in the middle third, a reconstructive plate with a number of holes from 6 to 8, plates were used for osteosynthesis. Plates with a hook for osteosynthesis of lateral comminuted fractures and dislocations of the clavicular-acromial joint were used in 8 patients, one patient had a plate fracture. With stable osteosynthesis of the clavicle, there was no need for additional plaster fixation of the upper limb. Functional rehabilitation, despite immobilization, began from the first postoperative day.Clinical example. ♀, 34 years old, household injury. Diagnosis at admission: closed fracture of the middle third of the left clavicle with displacement of fragments (Figure 1). Was performed extraosseous osteosynthesis with a reconstructive plate. Further dynamics were unremarkable, after 6 weeks a fracture union was achieved. The metal structure was removed after 1 year. The recovery of the function of the shoulder joint was complete.
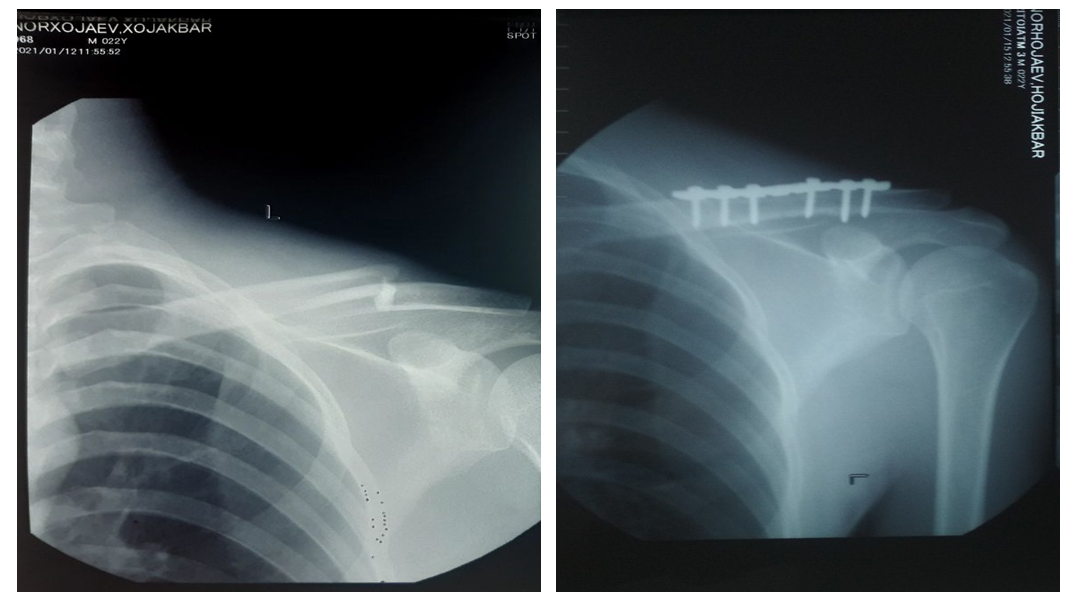 | Figure 1. X-rays of the clavicle in direct projection of patient K. before and after surgery |
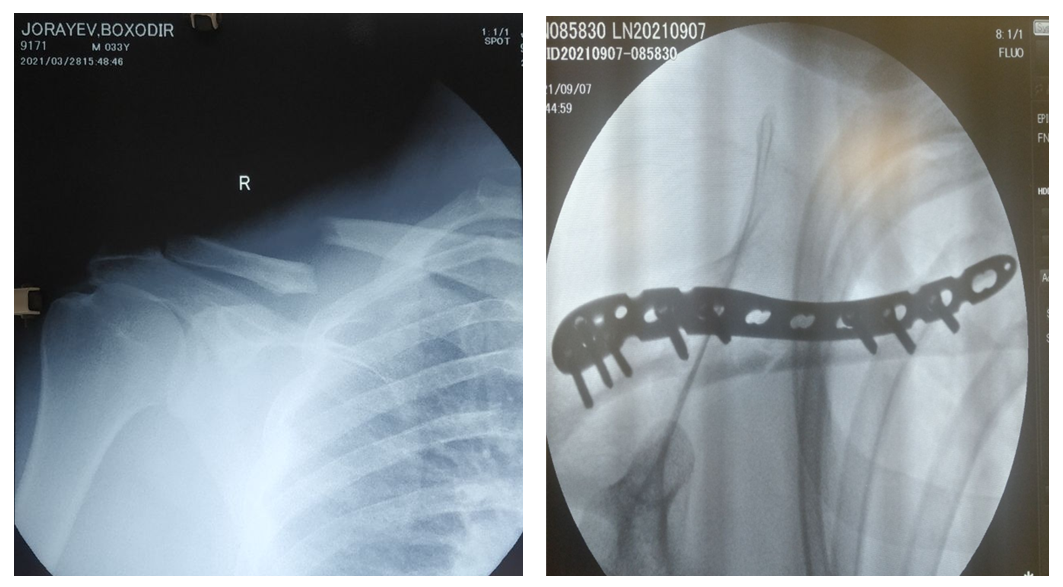 | Figure 2. Radiographs of the clavicle in direct projection. Patient K. before and after surgery |
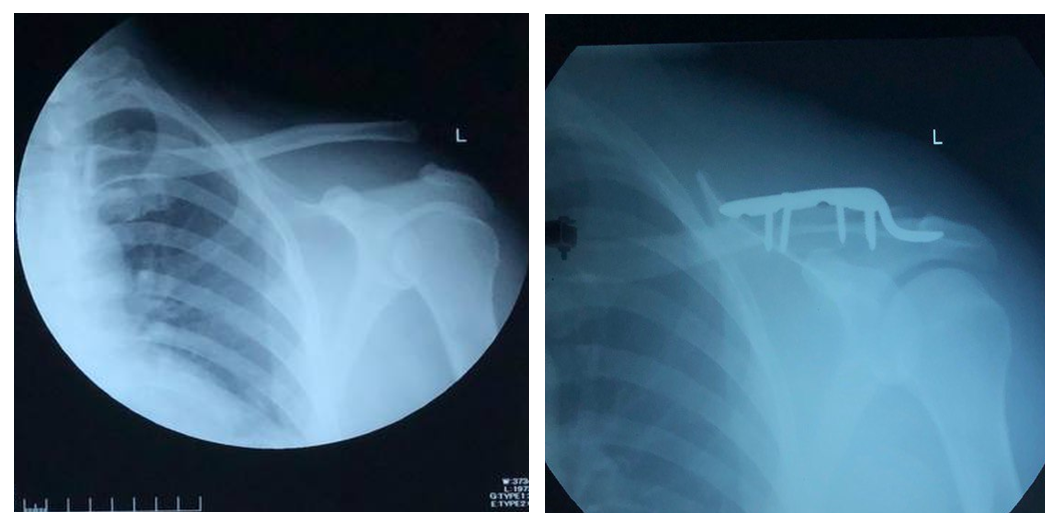 | Figure 3. Radiographs of the clavicle in direct projection. Patient K. before and after surgery |
4. Results
- In a comparative study of the results of treatment, depending on the methods of treatment, the following complications were observed: in the first group with intraosseous osteosynthesis with Ilizarov wires, the least traumatic, simple and accessible, intramedullary fixation with a thin (1.5, 2.0 mm) wire did not provide sufficient stabilization of fragments and patients , after the operation, needed external immobilization. The total bed-day was 11.3 ± 0.82, the postoperative bed-day was 7.89 ± 0.43.Bolnoy Kholbaev 38years.
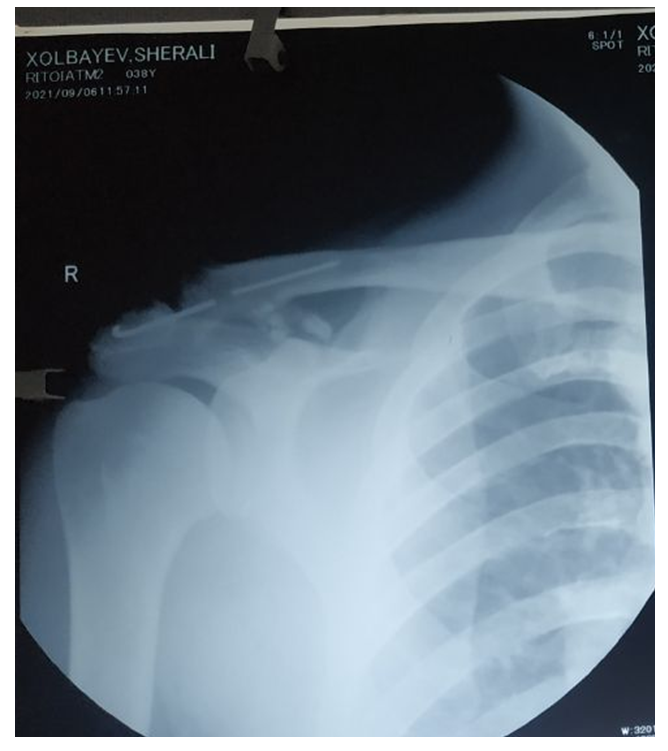 | Figure 4. Radiographs of the clavicle in frontal projections |
5. Conclusions
- Thus, bone osteosynthesis with the AO plate is, according to indications, modern high-tech, functionally beneficial and minimally invasive methods in the treatment of patients with fractures and fracture-dislocations of the clavicle. To prevent complications in osteosynthesis of fractures and fracture-dislocations of the clavicle, it is important not only to comply with treatment standards, but also to have technological provision with implants of various shapes and sizes and require a differentiated and individual approach to their treatment, depending on the nature and location of clavicle fractures.