-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(10): 714-717
doi:10.5923/j.ajmms.20211110.10
Received: Sep. 25, 2021; Accepted: Oct. 25, 2021; Published: Oct. 30, 2021

Clinical Outcomes of a Dental Education Program for Primary School Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMukhiddin Nizomiddin Ogli Saydaliev
Postgraduate Student of the Department of “Pediatric Therapeutic Dentistry”, Tashkent State Dental Institute, Uzbekistan
Correspondence to: Mukhiddin Nizomiddin Ogli Saydaliev, Postgraduate Student of the Department of “Pediatric Therapeutic Dentistry”, Tashkent State Dental Institute, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To study the effectiveness of a dental educational program for the prevention of dental caries and periodontal disease in children of primary grades. Material and methods: The object of the study was 175 junior schoolchildren of secondary schools №240, №259 and №302 in the city of Tashkent. The subject of the study was a dental education program, “A Dazzling Smile for Life”. Results: As a result of the educational dental program, the increase in caries was not observed in primary schoolchildren, after a year the intensity of dental caries according to the CSR index decreased from 4.13 + 0.23 to 3.09 + 0.20 p <0.05, the PMA index improved and was 15.7 + 0.77 p <0.05.
Keywords: School children, Hygienic index, Dental caries, Oral cavity, Dental diseases, Prevention programs, Dental status, Caries intensity
Cite this paper: Mukhiddin Nizomiddin Ogli Saydaliev, Clinical Outcomes of a Dental Education Program for Primary School Children, American Journal of Medicine and Medical Sciences, Vol. 11 No. 10, 2021, pp. 714-717. doi: 10.5923/j.ajmms.20211110.10.
Article Outline
1. Introduction
- In many countries, significant progress has been made in reducing the prevalence and intensity of dental caries in children [1]. The Global Databank of the Epidemiology of Caries documents large differences in the intensity of dental caries (Caries Seal Removal - CSR) of the key age group of 12 years [2,4], which are difficult to explain in terms of targeted control of this disease through the implementation of community prevention programs.For example, in China, a low level of caries intensity in children has been maintained for many years [11]. While in most countries of Western Europe during this period there was both a peak of carious disease (in a number of countries of the SCR teeth of 12-year-old children reached the level of 8-10 units), and a fantastic decrease in the prevalence and intensity of caries to the level of rare cases among children school age [14].
2. The Main Findings and Results
- Systematic monitoring of the dental health of the population is one of the most important components of the dental care system [12]. In a number of EU countries, there are automated programs for the annual registration of the main criteria for the dental status of children and the preventive measures taken [8,6,3]. In the countries of Eastern Europe, state systems for monitoring the dental health of the population according to the criteria recommended by the World Health Organization are in their infancy, but for more than 50 years information on the prevalence of dental diseases has been available in published scientific studies. Unfortunately, the results of this huge and important work of research institutes and dental departments of medical universities are practically not taken into account in the reporting systems of health authorities. It is quite difficult to eliminate this problem, since the ideal system for monitoring dental health on the example of Denmark [13] costs many times more than the entire system of dental care for children in Belarus or other CIS countries. A rational way out of this situation can be the use of non-costly information systems, for example, EGOHID-2005 (European Global System of Dental Health Indicators), developed by the European Commission on Health [9].Our experience of using this system in several countries has been positive [5,7,10]. An important aspect of these works was the identification of the determinants of dental caries and periodontal diseases, which makes it possible to substantiate evidence-based recommendations for optimizing the prevention and quality of treatment of major dental diseases.Thus, the relevance of this study is determined by the high prevalence of dental diseases and the possibility of obtaining a medical and social effect when carrying out scientifically based measures to form a high level of motivation in primary school children to maintain oral health.
3. Purpose of the Study
- To develop and evaluate the effectiveness of the prevention program "Dazzling smile for life" in order to preserve and strengthen the health of children of primary school age, the city of Tashkent.
4. Research Objectives
- To study the dental status of primary school children at baseline and in dynamics after 6 months and one year after the program.Evaluate the effectiveness of the “Dazzling Smile for Life” program for children of primary school age.
5. Materials and Methods
- The object of the research was the junior schoolchildren of educational institutions (175 people). The subject of the research was a dental educational program conducted in 2-3 grades of secondary schools №240, №259 and №302 in the city of Tashkent.Children participating in the educational program were included in the main group (84 people). Children, for whom the educational program was not carried out, made up a comparison group (91 people).In this article, we will focus on the change in clinical indicators in children obtained as a result of the implementation of this program.The participants in the study were persons whose legal representatives signed a voluntary informed consent. Dental examination of children was carried out using a set of dental instruments under artificial lighting.The clinical studies carried out as a result of the work were: examination, determination of the prevalence of caries, determination of the intensity of caries by the CSR + cs index, the hygienic state of the oral cavity was determined by the index of oral hygiene (Fedorova Volodkina) and the state of the periodontal soft tissues was studied by the PMA index (Parma).For statistical data analysis, the Statistica software package, developed by StatSoft, was used, which implements the functions of data analysis, data management, data visualization using statistical methods, as well as economic, statistical and graphical tools of the Microsoft Excel program, which is part of Microsoft's Microsoft Office.To estimate the mathematical expectation of the mean values of all parameters, interval estimation was performed. The values of continuous quantities are presented in the form M ± m, where M is the estimate of the mathematical expectation for the sample (sample mean), m is the parameter of the confidence interval (standard error of the mean).
6. Results and Discussion
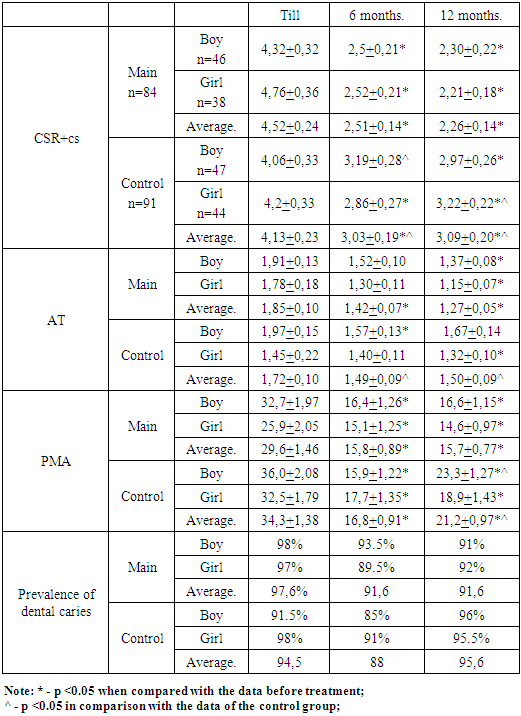
- As can be seen from the table, - the prevalence of dental caries after 6 months. after the application of the educational program decreased from 97.6 to 91.6%, the increase in the prevalence of caries was not observed. Under the influence of the preventive program during the year, the prevalence of dental caries reached 88.4%, an increase in the prevalence of dental caries in 12 months, amounted to 0%.By the end of the year, the prevalence of decay dental caries in children of the FD who did not participate in the prophylactic program was higher (95.6%) than in children participating in the program”.We also studied the change in the intensity of dental caries in children of the main group after 12 months. Applications of the program. As can be seen from table 1, the intensity of dental caries 6 months after the start of the lessons according to the CSR+cs indices was 2.51 ± 0.14. A year later, there was a decrease in the intensity of caries according to the CSR+cs indices to 2.26 ± 0.14 (P <0.001). There was no increase in intensity in the prophylactic group during the year of prophylaxis.
|
7. Conclusions
- As a result of the educational dental program, primary schoolchildren did not have a newly identified carious process, in comparison with the comparison groups of the same territories; a decrease in the hygienic indicator (improved hygiene) was noted in all territories in the groups of children of participants in the school educational program, in contrast to the comparison groups; the indicator of the interval of visiting a dentist by children in the dynamics of the educational program also significantly decreased in the main groups of the above territories. The results obtained by us testify to the achievement of the set goal and the fulfillment of the designated tasks.