-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(10): 678-682
doi:10.5923/j.ajmms.20211110.04
Received: Sep. 4, 2021; Accepted: Oct. 14, 2021; Published: Oct. 30, 2021

Treatment of Neurosensoral Death Combined with Stable Voltage Stenocardia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. S. Arifov1, D. A. Kalandarova1, 2
1Center for the Development of Professional Qualifications of Medical Workers of Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
2Republican Clinical Hospital No. 2 of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
Correspondence to: S. S. Arifov, Center for the Development of Professional Qualifications of Medical Workers of Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan.
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to evaluate the clinical and audiological results of the use of the drug Ginkgo biloba in the treatment of patients with sensorineural hearing loss (NDH), combined with stable angina pectoris functional class (FC) I - III. Comprehensive examination and treatment was carried out in 54 patients with NBT, combined with stable angina pectoris (FC I - III). The age of the patients ranged from 37 to 61 years (the average age was 44.4 ± 1.6 years). 41 patients, who underwent targeted treatment with NBT, constituted the main group. The other 13 patients who, for various reasons, were not treated with NBT, were combined into a comparison group. In patients with stable exertional angina pectoris I - III, hearing impairment manifests itself in the form of a lesion by the type of sound perception with a predominant lesion of the peripheral part of the auditory analyzer. After the course of treatment of patients with NBT, combined with stable exertional angina pectoris I - III with the use of the drug Ginkgo biloba, most of them showed an improvement in speech intelligibility, a decrease in the severity of tinnitus. At the same time, there was a significant improvement in the hearing threshold at two frequencies according to the data of tonal threshold audiometry in the usual frequency range, an increase in the registration of both classes of OAE to 19.5% of patients.
Keywords: Sensorineural hearing loss, Stable exertional angina, Ginkgo biloba
Cite this paper: S. S. Arifov, D. A. Kalandarova, Treatment of Neurosensoral Death Combined with Stable Voltage Stenocardia, American Journal of Medicine and Medical Sciences, Vol. 11 No. 10, 2021, pp. 678-682. doi: 10.5923/j.ajmms.20211110.04.
Article Outline
1. Introduction
- Cardiovascular diseases and changes in cerebral circulation occurring against their background are one of the significant etiological factors of sensorineural hearing loss (NDH) among the adult population [1-7]. In particular, our earlier studies revealed that in patients with coronary artery disease, angina pectoris, hearing impairment is formed by the type of sound perception with a predominant lesion of the peripheral part of the auditory analyzer. They indicated that the mechanism of development of hearing impairment ischemic heart disease, angina pectoris is realized through changes in cerebral circulation, which in turn leads to impaired activity in various parts of the auditory analyzer [8-10].To date, extensive experience has been accumulated in the treatment of patients with NBT. The variety of proposed methods and treatment regimens for NBT in the last decade once again suggests that none of the available methods gives absolute results [10-12].Despite the presence of a large body of scientific works devoted to the treatment of NBT with a combination of various diseases of the cardiovascular system, we have not encountered detailed studies devoted to the study of the effectiveness of drug therapy in patients with NBT, combined with stable exertional angina.The purpose of this study was to evaluate the clinical and audiological results of the use of the drug Ginkgo biloba in the treatment of patients with NBT, combined with stable exertional angina pectoris I - III.
2. Material and Research Methods
- Comprehensive examination and treatment was carried out in 54 patients with NBT, combined with stable angina pectoris (FC I - III). The age of the patients ranged from 37 to 61 years (the average age was 44.4 ± 1.6 years). Persons with concomitant chronic diseases of the CVS, central nervous system and other pathology of the hearing organ were not included in the development. 41 patients who underwent targeted treatment with NBT constituted the main group. The other 13 patients who, for various reasons, were not treated with NBT, were combined into a comparison group.The control group consisted of 20 healthy individuals.When diagnosing NBT, the International Statistical Classification of Diseases and Problems Related to Health, 10th revision (ICD-10) was followed.To assess the degree of hearing loss, the international classification of hearing impairments was used (WHO, 1997).The clinical diagnosis of stable exertional angina with the determination of its functional class (I - III) was made by a cardiologist based on the results of clinical, instrumental, and laboratory studies of the cardiovascular system.All patients underwent an assessment of the state of organs and systems of the body, examination of the ENT organs and a study of the auditory function. The nature, type and degree of hearing impairment was established using psychoacoustic and objective methods of hearing research. They consisted of studying complaints, medical history and life history, acumetry, tonal threshold audiometry, tonal threshold audiometry in an extended frequency range by air conduction, determining the differential threshold of sound intensity perception (Luscher test), speech audiometry, tympanometry, registration of delayed evoked otoacoustic emission (TEOAE) and Otoacoustic Emissions on Distortion Product (OAEPS).Statistical processing of the research results was carried out by the method of variation statistics, with the calculation of the mean square deviation and the arithmetic mean error by the method of moments (M ± m), the criterion for the reliability of Student's differences (t) and the degree of reliability (P).
3. Research Results
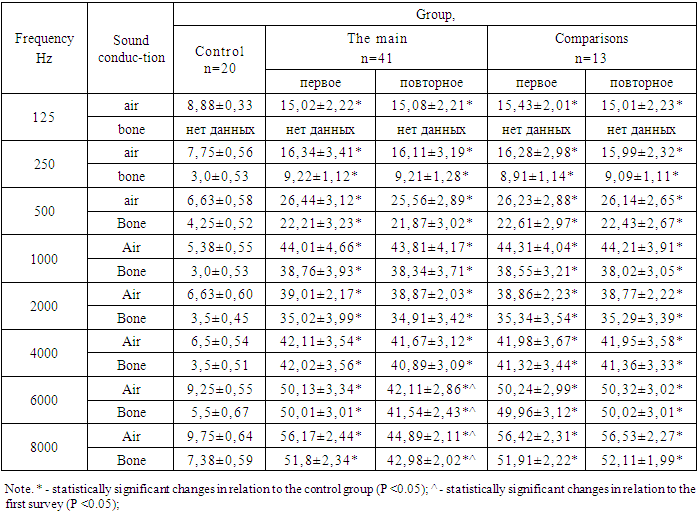
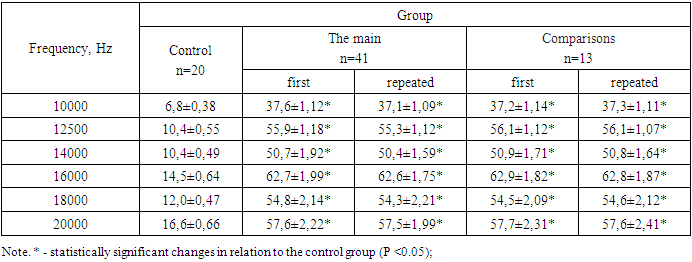
- Patients of the main group used the preparation Ginkgo biloba in order to correct disorders in the auditory analyzer. The drug was used at a dose of 120 mg / day with meals for two months. The choice of this drug was justified by the following facts:- there are many studies that indicate its effectiveness in the treatment of NBT of other etiology [13];- it has an effect on cerebral circulation, including on the rheological properties of blood and microcirculation, eliminates venous stasis, has an antihypoxic effect, affects neurotransmitter processes, in connection with which a nootropic, antidepressant effect is manifested [14-16];- in connection with the described multidirectional positive effect, there is no need to use several drugs, which is an important factor for patients with angina pectoris, who usually take several drugs on an ongoing basis.Patients in both groups received planned therapy for heart disease, according to the recommendations of the cardiologist.All patients underwent an assessment of the initial state of hearing during the initial examination. The result of treatment in patients of the main group was assessed one week after the end of taking the drug Ginkgo biloba. For the representativeness of the results, a repeated examination of the patients in the comparison group was carried out at the same time.In the main group, out of the total number of patients, 17 (41.5%) complained of noise, of which 13 (76.5%) had it bilateral and 4 had it on one side. In 15 (88.3%) patients, the noise was constant and 2 (11.7%) - periodic. In all, it had a high-frequency character. In the comparison group, tinnitus was noted in 46.2% of patients, and in all of them it was bilateral.After treatment in the main group, the number of patients with a complaint of noise decreased to 7 (17.1%). The nature of the manifestation of noise changed in a positive direction - in 5 (71.4%) patients the noise was constant and 2 (28.6%) - periodic, indicators of 90% and 10% before treatment, respectively. In the comparison group, tinnitus was noted by 46.2% of patients.Hearing loss in the main group was noted before treatment in 17 (41.5%) and after treatment in 12 (29.3%) patients. During the initial examination, 22 (53.6%) patients noted a decrease in speech intelligibility (9.1% constantly and 90.8% in a noisy environment, simultaneous communication of several people), and after treatment their number was 14 (34.1%). comparisons in two examinations, hearing loss was noted by 46.2% and a decrease in speech intelligibility in 53.8% of patients.According to the study using tuning forks in the main group, 21 (51.2%) and the comparison group 7 (53.8%) patients revealed characteristic hearing impairments by the type of sound perception. The result shows a relatively low diagnostic value of tuning forks. After treatment, this indicator was 20 (48.8%) in the main group and did not change in the comparison group.Tonal threshold audiometry in the usual frequency range revealed an increase in the thresholds of sound perception in all examined patients. In the main group, according to the results of audiometry in the usual frequency range, changes in hearing were detected in 26 (63.4%) patients. Of these, only 9 (22%) revealed varying degrees of hearing impairment by the type of sound perception based on the results of audiometry in the usual frequency range. Among them, in 7 patients, the first and 2 - the second degree of hearing loss was established, in 17 (41.5%) patients there was an increase in the thresholds of air and bone conduction in the high-frequency zone, and the average indicator of air conduction in them did not reach the value of the I degree of hearing loss (less than 26 dB). In 15 (36.5%) patients, an increase in thresholds relative to the age norm in the normal frequency range was not observed and hearing impairment was detected using tonal threshold audiometry in an extended frequency range, i.e., they had an increase in thresholds only in the ultrahigh frequency zone (10,000-20,000 Hz).Table 1 shows the results of tonal threshold audiometry in the usual frequency range of the studied patients in both groups. All patients showed a significant difference in air and bone conduction indicators over the entire frequency range compared to the control group.
|
|
4. The Discussion of the Results
- In patients with stable exertional angina pectoris I - III, hearing impairment manifests itself in the form of a lesion by the type of sound perception with a predominant lesion of the peripheral part of the auditory analyzer. Violation of intelligibility in the examined patients indicates the presence of violations in the central parts of the auditory analyzer. The results of this study showed a direct relationship between the severity of hearing disorders and FC of exertional angina in relation to the degree of hearing loss and the percentage of speech intelligibility. In severe cases, hearing and speech impairment were more pronounced. The development of hearing impairment with stable angina pectoris FC I – III is associated with impaired cerebral circulation, which has an adverse effect on the functioning, primarily of the peripheral and, in general, and other parts of the auditory analyzer. All this has a number of similar mechanisms as in the case of cerebral circulation disorders of a different nature [5,6].In the treatment of patients with NBT, combined with stable exertional angina pectoris I - III with the use of the drug Ginkgo biloba, a positive effect was achieved. After the course of treatment, the majority of patients showed an improvement in speech intelligibility, a decrease in the severity of tinnitus. At the same time, there was a significant improvement in the hearing threshold at two frequencies according to the data of tonal threshold audiometry in the usual frequency range, an increase in the registration of both classes of OAE to 19.5% of patients.
5. Conclusions
- 1. With sensorineural hearing loss in combination with stable angina pectoris FC I - III, the auditory analyzer has been affected throughout.2. In patients with sensorineural hearing loss in combination with stable exertional angina, pectoris FC I - III, Ginkgo biloba has been the drug of choice, which is due to its influence on most links in the mechanism of development of hearing impairment.