-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(8): 598-601
doi:10.5923/j.ajmms.20211108.11
Received: Aug. 15, 2021; Accepted: Aug. 26, 2021; Published: Aug. 30, 2021

Association of the Polymorphism rs1799998 CYP11B2 Gene with Left Ventricular Diastolic Function in Patients with Chronic Heart Failure
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNuritdinov N. A.
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Nuritdinov N. A., Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of our study was to evaluate the role of polymorphism rs1799998 CYP11B2 gene in patients with chronic heart failure (CHF). In patients with CHF 152 Uzbeks have been studied the alleles and genotypes rs1799998 CYP11B2 gene. A relationship has been established between the carriage of the homozygous T / T genotype of the rs1799998 polymorphism of the CYP11B2 gene with an almost twofold increase in the risk of the formation of a restrictive form of CHF, which allows us to make an assumption, regarding this genotypic variant, about its prognostic role in increasing the risk of developing this form of CHF.
Keywords: Chronic heart failure, rs1799998 CYP11B2, Gene
Cite this paper: Nuritdinov N. A., Association of the Polymorphism rs1799998 CYP11B2 Gene with Left Ventricular Diastolic Function in Patients with Chronic Heart Failure, American Journal of Medicine and Medical Sciences, Vol. 11 No. 8, 2021, pp. 598-601. doi: 10.5923/j.ajmms.20211108.11.
1. Introduction
- Chronic heart failure (CHF) is not only a medical, but also a social problem due to the significant prevalence, high mortality rate and high costs of treating patients with CHF. It is expected that in the next 20-30 years the prevalence of CHF will increase by 40-60% [1]. An increase in the activity of the sympathetic-adrenal system (SAS) and the renin-angiotensin-aldosterone system (RAAS) and other neurohormones, mediators, including cytokines, endothelin, natriuretic peptide system plays a leading role in the pathogenesis of CHF [2]. There are circulating and tissue RAAS in the body. The circulating RAAS (10-15%) as a "quick" response system provides a short-term influence and control over the cardiovascular system (CVS), and the tissue RAAS is a system of long-term regulation. Adaptive-compensatory reactions at the initial stage of CHF development are provided mainly by the circulating RAAS. With prolonged activation in CHF, tissue RAAS is also significantly activated, including myocardial and renal [3]. If the main link of the RAAS is angiotensin II (AT II), then aldosterone is an equally important link and its adverse effects, in many respects similar to the effects of AT II. The secretion of aldosterone is influenced by AT II, sodium and potassium levels, ACTH, vasopressin, natriuretic peptide and endothelin. Aldosterone is synthesized not only in the adrenal cortex, but also in the myocardium and in the vascular endothelium. Aldosterone promotes tissue fibrosis through several mechanisms: induction of inflammation and fibrinoid necrosis of small arteries and arterioles; effects on the corresponding receptors localized in the cytosol of vascular fibroblasts; stimulation of apoptosis of cardiomyocytes [4,5]. Aldosterone synthetase is a human enzyme encoded by the CYP11B2 gene (cytochrome P450, family 11, subfamily B, polypeptide 2) on chromosome 8. Aldosterone synthase belongs to the cytochrome P450 superfamily and provides the synthesis of the hormone aldosterone. The gene for aldosterone synthetase is mapped to chromosome 8 at q24.3. It is located next to the 11beta-hydroxylase gene (CYP11B1). The CYP11B2 gene is highly homologous to the CYP11B1 gene encoding 11-beta-hydroxylase. Despite significant research efforts, it is still unclear how the C-344T polymorphism affects steroid biosynthesis at the molecular level. On chromosome 8q24, the genes encoding the aldosterone synthase CYP11B2 and 11B-hydroxylase CYP11B1 are located in close proximity [6]. The most fully investigated polymorphism of the aldosterone synthase gene, which manifests itself in the substitution of cytosine for thymine at the 344th position of the nucleotide sequence, in the regulatory region of the gene. This site is the binding site for the steroidogenic transcription factor SF-1, which regulates the expression of the aldosterone synthase gene. According to recent studies, the T allele leads to an increase in aldosterone production, which in turn is associated with hypertension, as well as with fibrosis and myocardial hypertrophy and with the risk of hypertensive complications of pregnancy. A relationship was found between the aldosterone synthetase gene polymorphism and the size, weight, and diastolic function of the LV in young people. The aldosterone synthase gene has been assigned to candidate genes in the development of cardiovascular remodeling [7,8].The aim of our study was to association of the polymorphism rs1799998 CYP11B2 gene with left ventricular diastolic function in patients with chronic heart failure (CHF).
2. Materials And Methods
- In patients with CHF 134 of Uzbek nationality have been studied the genetic determinants of alleles and genotypes rs1799998 CYP11B2 gene. The control group consisted of 102 healthy individuals— men of Uzbek nationality. The study was performed according to the standards of Good Clinical Practice (Good Clinical Practice) and the Declaration of Helsinki. The study protocol was approved by the ethics committees of all participating clinical centers. Before inclusion in the study all participants provided written informed consent. All patients were divided into three groups of functional class (FC) of CHF according to the New York Heart Classification (NYHA) according to the test of 6-minute walk: the first group consisted of 31 patients with CHF FC I, the second group 62 patients with FC II and 3 group — 59 patients with FC III classification NYHA. Study polymorphism rs198389 NPPB gene was conducted using polymerase chain reaction on programmable thermocycler CG-1–96 «Corbett Research» (Australia) and 2720 «Applied Biosystems» (USA), using kits LLC “Medlab” (St. Petersburg), according to the manufacturer’s instructions. In our work allele polymorphism G/T894 revealed after digestion of the amplified fragment of 206 bp containing the polymorphic site. Evaluation of deviation of the distribution of genotypes of studied polymorphisms of DNA from the canonical distribution of Hardy-Weinberg equilibrium was performed using the computer program for the analysis of genetic data “GenePop” (“Genetics of Population”). To calculate the “odds ratio” (OR — odds ratio) with 95% confidence intervals (CI— confidenceinterval), χ2 and pvalues used statistical package statistical software package «OpenEpi 2009, Version 2.3».
3. Results
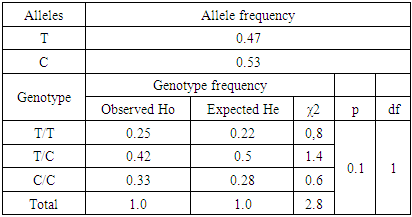
- Analysis of the frequency distribution of the genotypes of the rs 1799998 polymorphism of the CYP11B2 gene in the group of CHF patients showed a congruence for RHV. In particular, the frequencies of the C and T alleles were 0.47 and 0.53, while the observed frequencies of the C / C, C / T and T / T genotypes corresponded to 0.25; 0.42 and 0.33, and their expected frequencies were 0.22; 0.5 and 0.28 with a statistically insignificant difference (χ2 = 2.8; p = 0.1) and a heterozygosity index (D) equal to -0.16 (Table 1).
|
4. Discussion
- Aldosterone - a mineralocorticoid, which is mainly synthesized by the glomerular zone of the adrenal cortex from deoxycocorticosterone by the mitochondrial cytochrome p450 enzyme aldosterone synthetase increases the number of ATII type 1 receptors in the cardiovascular disease and potentiates the effects of RAAS. Aldosterone synthesized by the adrenal cortex mainly affects receptors located in the region of the distal renal tubules, the collecting ducts of the nephrons. By binding to intracellular mineralocorticoid receptors (type 1 corticoid receptors), aldosterone interacts with hormone-sensitive DNA elements and modulates the transcription of specific proteins [9]. At the same time, in recent years, the idea has been formed that aldosterone is synthesized not only in the adrenal cortex, but also in the myocardium, vascular endothelium, brain tissue and exerts its effect directly at the site of synthesis. It has been shown that aldosterone receptors are expressed on cardiomyocytes, endothelial cells, and human heart fibroblasts. Through activation of these receptors and possibly other, so far hypothetical, mechanisms, aldosterone increases collagen synthesis and induces fibroblast proliferation [10].Studies have shown that the activity of the RAAS is to a certain extent controlled at the genetic level and the functional significance of the RAAS in the processes of changing the geometry of the heart from the standpoint of molecular genetics is probably due to the level of AT II production, which in turn partially depends on the expression of the renin, angiotensinogen and ACE genes. aldosterone, as well as the density and functional activity of receptors present in the myocardium and blood vessels, because [11].
5. Conclusions
- Thus, the data obtained show a high frequency of occurrence of the T allele and the T / T genotype in the main group of patients compared to the control group by 1.2 and 1.6 times, which proves the presence of a tendency on their part to increase the risk of the formation of disorders leading to the development of CHF. A relationship has been established between the carriage of the homozygous T / T genotype of the rs1799998 polymorphism of the CYP11B2 gene with an almost twofold increase in the risk of the formation of a restrictive form of CHF, which allows us to make an assumption, regarding this genotypic variant, about its prognostic role in increasing the risk of developing this form of CHF.