Sh. M. Kamalova1, E. A. Kharibova2, Sh. J. Teshaev2
1Anatomy Department, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Anatomy, Clinical Anatomy (OSTA) Department, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Sh. M. Kamalova, Anatomy Department, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The study involved 136 children with scoliosis. Using the method of 3D computer photometry with graphic-analytical interpretation of the image and system analysis, such anatomical parameters as length, width, angle of the 1st and 5th fingers, heel angle were obtained. An automated complex has been developed for screening and express diagnostics of flat feet in children with scoliosis.
Keywords:
Flat feet, Foot, Scoliosis, Digital photometry, Computer plantography
Cite this paper: Sh. M. Kamalova, E. A. Kharibova, Sh. J. Teshaev, Changes in Anatomical Parameters of the Feet in Children of the First and Second Periods of Childhood with Scoliosis, American Journal of Medicine and Medical Sciences, Vol. 11 No. 7, 2021, pp. 542-546. doi: 10.5923/j.ajmms.20211107.09.
1. Introduction
1.1. The Relevance of the Problem
Scoliosis is called a biological tragedy of humanity. With scoliosis, there are violations not only of the functions of the musculoskeletal system [1]. The problem of functional diagnosis of foot injury and disease is relevant in the choice of tactics and methods of treatment and evaluation of its effectiveness. Among the various deformities of the lower extremities, the most common is flat feet, characterized by flattening of the longitudinal and transverse arches of the foot in combination with rotation around the longitudinal axis, as well as its withdrawal. The predominance of flat feet in the structure of foot pathology indicates the need to improve the methods of diagnosing this condition. Early diagnosis of flat feet is very important when conducting dispensary examinations of children in preschool and school educational institutions, in sports medicine, for the timely prediction of athletes ' health disorders [2].From the available literature sources, it is known that the longitudinal arch of the foot and its spring function in children are formed by the end of the 4th year of life [3]. However, we assume that the longitudinal arch of the foot continues to form in subsequent age periods.Diagnosis of foot pathology is traditionally based on several non-automated methods: visual, podometric, X-ray, plantographic, etc. In recent years, automated diagnostic methods have been increasingly used to assess the height of the arch of the foot and the degree of its flatness. In particular, there is a technique that allows you to assess the nature of foot deformity using strain-gauge platforms. However, the latter method requires the manufacture of a special device containing a matrix of load cells, which complicates the design of the diagnostic device. Another technique uses a foot image obtained using a flatbed scanner with a CCD sensor. However, this technique does not allow us to assess the nature of changes occurring in different parts of the foot [4].
1.2. The Aim of the Study
The goal of the study was to develop an automated system for screening and rapid diagnosis of flat feet in children with scoliosis.
2. Materials and Research Methods
In this work, a new method for diagnosing flat feet has been successfully tested, based on the analysis of foot images obtained using an upgraded software and hardware complex (PAC) for assessing the morphofunctional state of the human body (digital 3D photometrograph).The image of the foot was obtained using a computer photoplantograph using the technology of projection transposition photometry, the body of which is reinforced and able to withstand the weight of the human body. The measurement is performed in a standing position. The subject puts both feet on the surface of the 3D computer photoplantograph first, and then alternately each one separately, the object (foot) is photographed sequentially from all sides (front, back, sides, top), which allows you to get the required number (6 pcs.) of rating images with minimal preliminary positional and manual marking.The developed diagnostic program analyzes the obtained images of the foot by the graphoanalytic method, which is widely used in medical practice. In this case, the program selects several key points on the image of the foot, and then calculates the distances between the points, as well as the angles by which the degree of longitudinal and transverse flat feet is determined. The diagnostic results are displayed on the screen and can be exported to the Microsoft Word word processor for later saving and printing.The program allows you to determine the condition of various parts of the foot. The condition of the forefoot is characterized by the following indicators: the angle of NAP-deviation of the 1st finger (if the angle of NAP is less than 18°, then the medial part of the foot is normal; with NAP more than or equal to 18°, there is a transverse spreading); the angle of QBR-deviation of the 5th finger (if QBR is less than 12°, then the lateral part of the foot is normal, while with QBR more than or equal to 12°, there is a transverse spreading). The condition of the middle part of the foot is characterized by the indicator K, where K = X / Y, where X is the width of the painted part of the print along the line VV’, Y is the width of the outer part of the longitudinal arch of the foot. The degree of longitudinal flatfoot is determined by the K indicator as follows: at K ≤ 0.5 - the foot is hollow; at 0.5 < K ≤ 1.10 - the foot with a normal arch; at 1.10 < K ≤ 1.20 - the foot with a reduced arch; at 1.20 < K ≤ 1.30 – the first degree of flatfoot; at 1.30 < K ≤ 1.50 - the second degree of flatfoot; at K > 1.50 - the third degree of flatfoot. The condition of the posterior part of the foot is characterized by the calcaneal angle HC'K: if the angle is greater than or equal to 5°, the condition of the foot is normal, whereas if it is less than 5° – the foot is flat.The length of the anterior and posterior sections, cut off by the lines WW' and UU', respectively. If these sections are elongated, it means that the foot is flat even in the normal state of the middle section.The method presented above for determining the state of the foot, identifying and evaluating possible manifestations of transverse and longitudinal flat feet was the basis for the computer diagnostic method used in this work. Figure 1 shows the program window for calculating the morphofunctional state of the foot.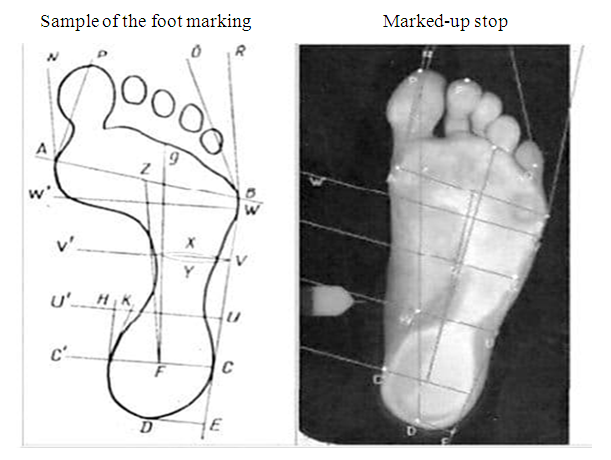 | Figure 1. The program for calculating the anatomical and functional parameters of the foot |
Analyzing the print obtained on the monitor screen, it becomes clearly noticeable that the surface of the foot adjacent to the scanner surface looks lighter in the image. Thus, there is enough information in the image of the foot to get the area of the surface of the foot adjacent to the scanner. To determine the area, the program uses the definition of the foot contour and counting the points lying inside the contour [5,6,7]. Each of the sections of the supporting surface of the foot is highlighted by the program in its own color (Fig. 2).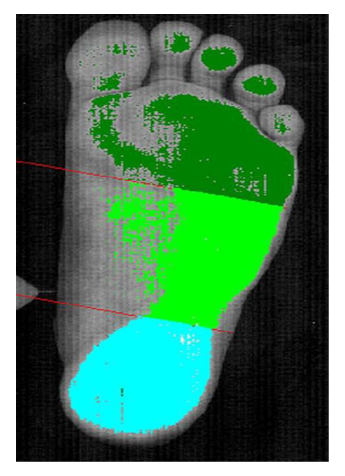 | Figure 2. Determination of the area of the supporting surface of the entire foot and its parts |
The analysis of the dynamic (time) series was reduced to the calculation of the following indicators: absolute growth (or decrease); growth rate (or decrease); growth rate. The absolute increase is the difference between the next level and the previous level. The growth rate is the ratio of the next level to the previous one, multiplied by 100%. The growth rate is the ratio of the absolute increase (decrease) to the previous level, multiplied by 100%.According to the above method, a morphofunctional study of the feet was performed in 136 children with scoliosis. 83 girls and 53 boys aged from 3 to 12 years were examined.
3. The Results of the Study
The anatomical and functional parameters of the foot identified by us in children with scoliosis are grouped in the table.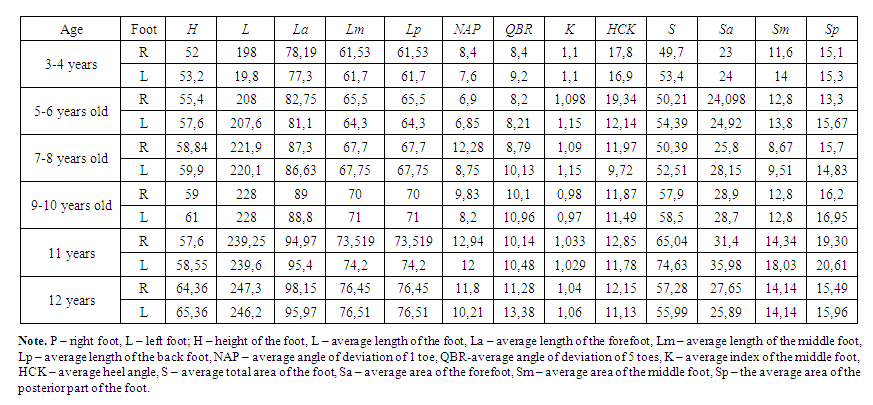 | Table 1. Indicators of the morphological state of the foot in children with scoliosis |
In male rats of 90 days of age in the control group, the body weight varied between 95,6 ± 120,3 g and in average 106,8 ± 1,53 g. Testes are oval and are mainly found in the scrotum, less often in the inguinal-scrotal canal. The mass of the testes varies individually from 0.62 g to 0.88 g, on average 0.78 ± 0.016 g. The relative weight of testes was 1,46%. The length of the testes is 1.23 - 1.78 cm, on average 1.42 ± 0.034 cm. The width of the testes ranges from 0.9 to 1.3 cm, an average of 1.11 ± 0.025 cm. The volume of testes individually ranges from 0.61 to 0.83 cm3, an average of 0.69 ± 0.014 cm3. Microscopic examination of testicular tissue sections showed that, at this age, the diameter of the convoluted seminiferous tubules increases, a free lumen appears to promote mature sperm, so the density of the testis tissue decreases sharply.The medial part of the forefoot in all children aged 3-4 years was within the normal range. At the same time, there was a deviation of 5 toes, exceeding the normal values. Among children aged 3-4 years, 10 (32.3%) people had a deviation of the 5th toe over 12°, which indicated a flattening of the lateral part of the forefoot. At the same time, 3 people had bilateral changes. In most cases, changes in the 5th finger were observed on the left. More pronounced changes were observed in the middle part of the foot. The K coefficient indicated a decrease in the arch of both feet in 7 (22.6%) people. Unilateral reduction of the foot was observed in 15 (48.4%) people. The first degree of flat feet on both sides was not detected in any person. In 9 people, the first degree of this pathology was unilateral. Only 1 person in this age group was found to have grade III flat feet on one side. The condition of the posterior part of almost all children was assessed as normal, only in 1 child the angle of the HC'C was less than 5°, which indicated valgation of the calcaneus. In 5-6-year-old children, the following changes were detected in the anterior part of the foot: deviation of 1 finger above the norm was observed in 1 person, while the QBR angle (deviation of 5 finger) was more than 12° in 6 (30%) people, and only in 1 – on both sides. Pathological changes in the middle part of the foot were more pronounced: a decrease in the arch of the foot was observed in 9 people (one of them on both sides), I degree of flat feet on one side in 3, 11 degree – in 4 (one of them on both sides) and III degree of deformity on one side was detected in 1 child. Changes in the posterior part of the foot in this age group did not go beyond the normal parameters. Among children of 7-8 years of age, changes in the anterior part of the foot in the form of an increased deviation of 1 toe outwards on one side were detected in 2 people. 3 children had a deviation of 5 toes, and 1 of them had a bilateral deviation. These changes indicated a transverse flattening of the forefoot. Changes in the middle department were observed in 13 people, only in 1 case 1 the process was two-sided. In 11 children, there was a decrease in the longitudinal arch of the foot, in 2 children, flat feet of the I degree and in I–II degree. Valgization of the calcaneal angle was detected in 3 children, only in 1 person – on both sides.In 9-10-year-old children, deviations of the medial part of the foot were not detected. In the lateral part of this part of the foot, only 1 child had changes indicating the first degree of transverse flatfoot. No changes were detected in the middle and posterior parts of the foot.In 11-year-old children, there were pronounced changes in the anterior part of the foot: in its medial part: flat feet of the first degree were detected in 5 (25%) people, of them on both sides – in 2, II degree – in 2 (10%) people, and only one on both sides. In the lateral part of this part of the foot, I degree of flat feet was detected in 11 (55%) people, 5 of them on both sides, II degree of flat feet – in 11 (55%), 4 of them had bilateral pathology. In the middle part of the foot, a slight decrease in its arch occurred in 9 (45%) people, in 3 the process was bilateral. Valgation of the calcaneal angle was observed on one side in 2 people.Among 12 – year – olds, in the medial part of the anterior part of the foot, 9 (27.3%) people had grade I flat feet, of which only 1 had two sides, and grade II on one side – in 3. In the lateral part of the anterior part, grade I flat feet were detected in 17 (51.5%) people, of which 6 had two sides. Grade II flat feet in this part of the foot occurred in 23 (69.7%) people, and 14 (42.4%) of them had pathology on both sides. In 18 children of this age, there was a decrease in the arch of the foot in the middle part, and in 6 people the process was localized on both sides. Reducing the NS angle’K less than 5° was observed in 7 children, and in 2 people on both sides. In children aged 3 to 12 years, there is a gradual increase in the length of the foot. The rate of increase in foot height in children with scoliosis is noted from 3 to 6 years, then up to 11 years, the height of the foot remains unchanged and only at 12 years there is a further increase in foot height.The growth dynamics of the anterior part of the left foot in children aged 3 to 12 years slightly outstrips the growth rates of the same part of the foot of the opposite limb. The same growth rates of the middle and posterior parts of the foot are noted. With the process of age in children with scoliosis, there is an increase in the deviation of both 1 finger outwards and the reduction of 5 fingers. The largest deviation of 1 finger was observed on the left in children aged 7-8 years, and 5 fingers on the right-in children aged 12 years. With age, the number of patients with deformity of the anterior-medial part of the foot increases sharply, if at the age of 5-6 years 1 person with flat feet of the first degree is detected, then by the age of 12 there are already 12 people, 3 of them with the second degree. The number of children with deformity of the antero-lateral part of the foot also increases during growth. So if in 3-4 years the deviation of the 5th toe above the normal value was noted in 10 people, then by 12 years-already in 34, and the majority had the II degree of deformation.In children with scoliosis, during their growth, there is a decrease in the K coefficient, which indicates the state of the longitudinal arch of the foot in its middle section. So, if in 3-4-year-olds this indicator is 1.1 for both feet, then by the age of 12-1.04 on the left and 1.06 on the right. A change in this indicator indicates an increase in the longitudinal arch of the foot in children with scoliosis.The number of children with longitudinal flat feet decreases with age. If at the age of 3-4 years, changes in the middle part of the foot were observed in 32 people, then at 12 years – in 18.With age, there is a decrease in the angle of the NS'K. And if in 3-4 years it is on average 17.8° on the left and 16.9° on the right, then in 12 years-12.15° and 11.13°, respectively.The rate of increase in the average total area of the plantar surface of the foot in children with scoliosis from 3 to 8 years is insignificant, but by 9-10 years there is a certain jump, and an even greater increase occurs in 11 years of age.The total area of the plantar surface of the right foot in children from 3 to 11 years is greater than that of the left foot. The average area of the forefoot has similar trends. The average value of the area of the middle part of the foot in children from 3 to 8 years old decreases, then it gradually increases with the achievement of maximum indicators at the age of 11 years. The rate of changes in the average area of the posterior part of the foot is not so pronounced. The increase in this indicator up to 9-10 years is not observed. The jump in the increase in the area of this department is observed only by the age of 11.
4. Discussion and Conclusions
The value of the K coefficient in the asthenic body type in adolescents exceeds this value of the period of early childhood, which indicates a significant decrease in the longitudinal arch of the foot. Consequently, we see that the formation of the longitudinal arch of the foot, and hence its spring function, is adversely affected by belonging to the asthenic body type in men and to the hypersthenic body type in women.In children aged 3 to 12 years, there is a gradual increase in the length of the foot. The rate of increase in the height of the foot in children with scoliosis is noted from 3 to 6 years, then up to 11 years, the height of the foot remains without dynamics and only at 12 years there is a further increase in it. The growth dynamics of the anterior part of the left foot in children aged 3 to 12 years slightly outstrips the growth rates of the same part of the foot of the opposite limb. The same growth rates of the middle and posterior parts of the foot are noted. With the process of age in children with scoliosis, there is an increase in the deviation of both 1 finger outwards and the reduction of 5 fingers. The largest deviation of 1 finger was observed on the left in children aged 7-8 years, and 5 fingers on the right-in children aged 12 years. In children with scoliosis, during their growth, there is a decrease in the K coefficient, which indicates an increase in the longitudinal arch of the foot. In the course of age in children with scoliosis, there is a decrease in the angle of the NS'K, which indicates a tendency to valgization of the calcaneus.
References
| [1] | Kamalova Sh. M., Teshaev Sh. J. Comparative Characteristics of Morphometric Parameters of Children with Scoliosis // American Journal of Medicine and Medical Sciences, USA. - 2020. - №10 (9). - P. 725-727. |
| [2] | Perepelkin A. I. Plantographic indicators of the feet of girls aged 8-11 years with different physiques / K. V. Gavrikov, V. B. Mandrikov, S. V. Klauchek, A. I. Perepelkin, L. V. Zarapkin // Problems of diagnostics, strengthening and rehabilitation of the musculoskeletal system in athletes: A collection of materials of the international scientific and practical conference Volgograd, June 26-28, 2008-Volgograd: FGOU VPO "VGAFK", 2008. - pp. 32-34. |
| [3] | Gryaznukhin E. G., Klyuchevsky V. V. Injuries and diseases of the foot // Traumatology and orthopedics: A guide for doctors / Ed. N. V. Kornilov: In 4 volumes. St. Petersburg: Hippocrates, 2004. Vol. 3: Injuries and diseases of the lower extremity / Edited by N. V. Kornilov and E. G. Gryaznukhin. St. Petersburg: Hippocrates, 2006. pp. 542-575. |
| [4] | Kamalova Sh. M., Kharibova E. A. Changes in anthropometric parameters of physical development of children with scoliosis // Society and innovations. 2 (2021) pp. 432-440. |
| [5] | Kashuba V. A. Biomechanics of posture. - Kiev: Olympic literature, 2003. - 166 p. |
| [6] | Perepelkin A. I., Krayushkin A. I. Dynamics of linear parameters of the foot of girls with increasing load // Bulletin of the Volgograd State Medical University. 2013. No. 2. pp. 25-27. |
| [7] | Perepelkin A. I., Krayushkin A. I., Smaglyuk E. S., Suleymanov R. H. Research of the supporting surface of the foot in the youth age. 2011. Vol. 18, no. 2. pp. 150-152. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML