Akhmedova S. M., Rakhimova M. O., Adilbekova D. B., Xatamov A. I., Nisanbaeva A. O'.
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Akhmedova S. M., Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The characteristic of the growth rates of various indicators at the stages of screening examination allows us to judge the adaptation processes occurring in the process of fetal growth. And in fetuses of pregnant women in a state of hypothyroidism, the intensity of growth of head parameters was less compared with the parameters of fetuses of healthy pregnant women. In fetuses of pregnant women in a state of hypothyroidism, the biparietal head size is significantly smaller at the stage of the second screening examination than in fetuses of healthy pregnant women.
Keywords:
Hypothyroidism, Experimental hypothyroidism, Thyroid pathology, Thyroid gland, Fetal fetometry, Prenatal ontogenesis, Hypothyroid pregnant women, Fetal anthropometry
Cite this paper: Akhmedova S. M., Rakhimova M. O., Adilbekova D. B., Xatamov A. I., Nisanbaeva A. O'., Indicators of Fetometry of the Fetus in Pregnant Women in a State of Hypothyroidism, American Journal of Medicine and Medical Sciences, Vol. 11 No. 5, 2021, pp. 394-397. doi: 10.5923/j.ajmms.20211105.07.
1. Introduction
The physiological role of thyroid hormones is extremely great and diverse in all periods of a person's life, including intrauterine [1]. They regulate and coordinate the development of the fetus, the processes of growth and differentiation of tissues, especially the nervous one [3]. Thyroid hormones affect almost all metabolic processes, determine postnatal growth, psychomotor, physical and intellectual development [2,4]. The functioning of many organs and systems largely depends on how fully the child's needs for thyroid hormones are met [3]. An actively functioning thyroid system determines the level of the child's general health [5]. A complex of unfavorable factors, including, first of all, a complicated course of pregnancy, childbirth, diseases of newborns lead to a violation of the postnatal adaptation of the pituitary-thyroid system of newborns, which manifests itself in the form of a transient increase in the level of thyroid-stimulating hormone during the first month of life and is defined as neonatal transient hypothyroidism [3,7]. The course of pregnancy in women with various pathologies of the thyroid gland may be accompanied by intrauterine growth retardation, low birth weight, and antenatal death [6]. However, according to the literature, we did not find information about the anatomometric features of the fetus at different stages of pregnancy in women in a state of thyroid insufficiency. An in-depth study of this issue will make it possible to develop recommendations for a rational assessment of fetal development in this category of pregnant women.The aim of our study was to study the anthropometric parameters of the fetus in healthy and pregnant women in condition of hypothyroidism.
2. Materials and Research Methods
Mandatory screening tests in the I, II and III trimesters are performed in accordance with the order of the Ministry of Health of Uzbekistan of June 2018, PO - 5590 “On improving prenatal diagnostics in the prevention of hereditary and congenital diseases in children.” Fetometry data of 25 healthy fetuses and 32 fetuses in condition of hypothyroidism were determined. Screening studies were conducted according to the standard at a certain time: the first screening at 12-13 weeks, the second screening at 22-23 weeks, and screening in 22-23 weeks. The average age of pregnant women in both groups averaged 33 ± 0.4 years, all pregnant women had singleton pregnancies. Examination of pregnant women includes a mandatory three-time screening ultrasound examination: in 10-14 weeks of pregnancy, when the thickness of the collar space of the fetus is mainly assessed; in 20-24 weeks, ultrasound is performed to identify malformations and echographic markers of chromosomal diseases; ultrasound examination in 32 - 34 weeks is carried out in order to identify malformations with their late manifestation, as well as for the purpose of functional assessment of the state of the fetus. The main purpose of these studies is to assess the capabilities of the fetoplacental system in terms of providing appropriate conditions for the development of pregnancy and its successful completion.
3. Results of Our Own Research
The results of the study showed that the biparietal head diameter in fetuses of healthy pregnant women at the stages of the first screening examination in 12-13 weeks averaged 22.2 ± 1.3 mm, in fetuses of pregnant women in a state of hypothyroidism at the stages of the first screening examination did not differ significantly, and averaged 20.9 ± 1.4 mm (Fig. 1).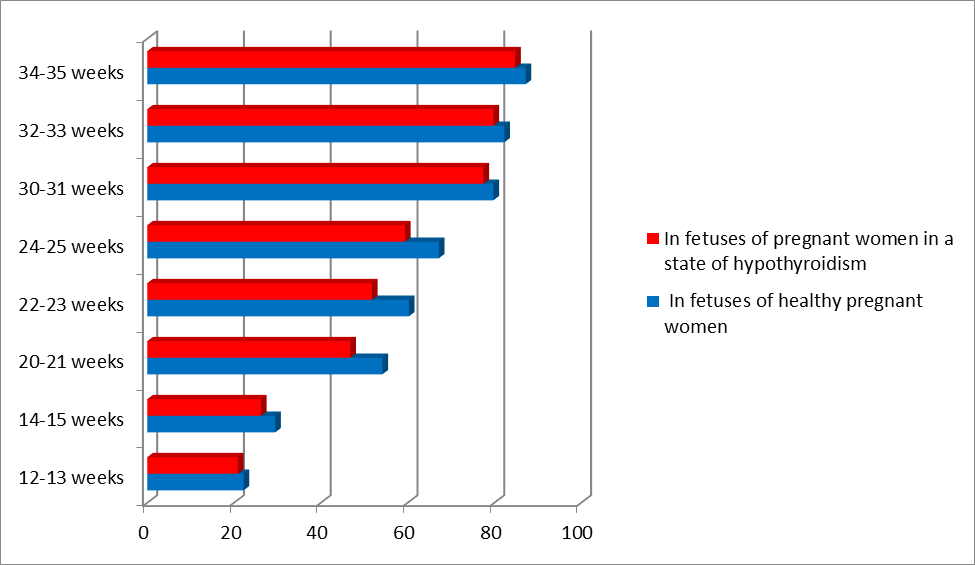 | Figure 1. Dynamics of changes in the indicator of the biparietal size of the fetal head |
In fetuses of healthy pregnant women in 14-15 weeks, the size of the biparietal indicator averaged 29.5 ± 0.8 mm, in pregnant women in hypothyroidism, this indicator was less and amounted to 26.2 ± 1.2 mm. The rate of increase in biparietal diameter indicators from 12 to 15 weeks in fetuses of healthy pregnant women was 32%, and 25.3% in fetuses of pregnant women in a state of hypothyroidism. At the time of the second screening examination, the biparietal diameter of the fetal head in pregnant women in a state of hypothyroidism was significantly less in comparison with the group of fetuses of healthy pregnant women. The average values of this indicator in fetuses of healthy pregnant women in 20-21 weeks was 54.2 ± 2.6 mm and in fetuses of pregnant women in hypothyroidism - 46.8 ± 1.4 mm.In 22-23 weeks, these indicators averaged 60.3 ± 2.6 mm in fetuses of healthy pregnant women and 51.8 ± 1.9 mm in pregnant women in a state of hypothyroidism. In 24-25 weeks -67.2 ± 2.6 mm and 59.4 ± 1.9 mm, respectively.Data analyzes have shown that the indicators of the biparietal diameter of the fetal head in healthy pregnant women are statistically significantly higher when compared with the values in pregnant women in condition of hypothyroidism. However, the growth rate of this indicator in fetuses of healthy pregnant women was 23.9% from 20 to 25 weeks, and 26% in fetuses of pregnant women in a state of hypothyroidism. Analysis of the data of the third screening examination shows that the indicators of biparietal diameter in pregnant fetuses were statistically significantly lower (p <0.05). During the third screening examination, the mean values of the biparietal diameter of the fetal head in healthy pregnant women were 79.8 ± 1.6 mm (at 30-31 weeks), 82.3 ± 1.5 mm (32-33 weeks) and 87.2 (34-35 weeks), respectively. In fetuses of pregnant women in a state of hypothyroidism, the average values of this indicator were 77.5 ± 0.7 mm in 30-31 weeks of gestation, 79.8 ± 1.2 mm in 32-33 weeks, and 84.8 mm in 34-35 weeks ± 0.8 mm respectively lower. Moreover, these indicators are 2% higher in fetuses of healthy pregnant women. In fetuses of healthy pregnant women in 12-13 weeks, the frontal occipital size averaged 27.3 ± 1.3 mm, this indicator in fetuses in 14-15 weeks was 35.9 ± 1.8 mm. The analysis of the data showed that the size of the fetal head of the frontal occipital indicators in pregnant women in a state of hypothyroidism is less and averaged 25.3 ± 1.5 mm in 12-13 weeks of gestation and 32.8 ± 0.9 mm in 14-15 weeks. In the data of these indicators, no significant differences observed (p> 0.05). The rate of increase in the frontal occipital size in fetuses of healthy pregnant women in the period from 12 to 15 weeks was 31%, in fetuses in a state of hypothyroidism was 29%. The frontal-occipital size of the fetal head in healthy pregnant women at the stages of the second screening examination averaged 65.9 ± 1.1 mm in 20-21 weeks, in 22-23 weeks these indicators reached an average of 72.8 ± 1.5 mm. In fetuses of pregnant women in a state of hypothyroidism, the dimensions of the frontal occipital size were slightly lower and averaged 60.8 ± 0.9 mm in 20-21 weeks, and by 22-23 weeks, they were 67.8 ± 1.3 mm. The indicators of the frontal occipital size of the fetal head in healthy pregnant women at the stages of the second screening examination in 24-25 weeks averaged 80.2 ± 1.2 mm, in fetuses of pregnant women in a state of hypothyroidism these indicators were statistically insignificant and amounted to -75.6 ± 1,0 mm, in 22-23 weeks these indicators reached an average of 72.8 ± 1.5 mm.During the third screening examination, the frontal occipital size in fetuses of healthy pregnant women in 30-31 weeks averaged 99.2 ± 1.5 mm, in fetuses in hypothyroidism these indicators were 99.0 ± 0.8 mm. In 32-33 weeks, the average values of the frontal occipital size of the fetal head were 104.9 ± 0.9 mm in healthy pregnant women, and 102.9 ± 1.3 mm in pregnant women in conditions of hypothyroidism. In 34-35 weeks, these indicators in fetuses of healthy pregnant women were 108.6 ± 1.5 mm, in the group of healthy pregnant women, 108.1 ± 1.1 mm. When comparing both groups, no statistical differences were found. At the time of the third screening examination, the growth rate of the frontal occipital size from 30 to 35 weeks in the group in fetuses of healthy pregnant women was 9.4%, and in fetuses of pregnant women in a state of hypothyroidism - 9.1%. Another criterion for assessing the development of the fetal skull is the size of the head circumference. The size of this indicator does not depend on the shape of the fetal head. In terms of 12-13 and 14-15 weeks (the period of the first screening examination), the average value of this indicator in fetuses of healthy pregnant women was 75.5 ± 1.4 mm and 100.3 ± 0.5 mm, respectively, and in fetuses in a state hypothyroidism 73.2 ± 1.1 mm and 96.9 ± 1.4 mm.There were no statistically significant differences in these values in the compared groups (p> 0.05). The growth rate of head circumference in fetuses of healthy pregnant women was 32.8%, and in fetuses with hypothyroidism - 32.3%.At the stage of the second screening examination in fetuses of healthy pregnant women in 20-21 weeks, the average head circumference reached 181.8 ± 1.8 mm, 199.3 ± 3.1 mm in 22-23 weeks and 220.0 ± 2, 7 mm in a period of 24-25 weeks. The average head circumference in fetuses with hypothyroidism at this stage of the survey was 177.5 ± 1.8 mm; 190.1 ± 2.5 mm and 215.3 ± 3.1 mm, respectively. The rate of increase in the size of the head circumference from 20 to 25 weeks in fetuses of healthy pregnant women was 21%, and in fetuses in a state of hypothyroidism 21.2%. At the stage of the third screening examination in 30-31 weeks in fetuses in a state of hypothyroidism, the head circumference was 280.2 ± 2.4 mm, in 32-33 weeks - 294.5 ± 2.1 mm, in 34-35 weeks - 305.9 ± 2.4 mm.In fetuses of healthy pregnant women, the head circumference was 281.4 ± 2.1 mm; 297.6 ± 2.5 mm and 312.4 ± 3.9 mm, respectively. The growth rate of the head circumference from 30 to 35 weeks in fetuses of healthy pregnant women was 11%, and in fetuses of pregnant women in a state of hypothyroidism - 9.1%. There were no statistically significant differences in these values in the compared groups (p> 0.05).The characteristic of the growth rates of various indicators at the stages of screening examination allows us to judge the adaptation processes occurring in the process of fetal growth. Analysis of our data shows that the period from 16 to 20 weeks (the stages between the first and second screening examinations) is the highest rate of increase in head size.At the same time, in fetuses of healthy pregnant women, the rate of increase in biparietal diameter was 83.7%, frontal-occipital size - 83.5%, head circumference - 81.2%.In fetuses of pregnant women in a state of hypothyroidism, the intensity of the growth of head parameters was less in comparison with the parameters of fetuses of healthy pregnant women. Thus, the biparietal head diameter in pregnant fetuses in a state of hypothyroidism for the period from 16 to 20 weeks of intrauterine development increased by 78.6%, the frontal-occipital size by 85.3%, and the head circumference by 75.7%.The increase in the parameters of the head of the fetuses of both groups from 21 to 25 weeks slowed down by 2 times. At the same time, indicators of biparietal head diameter in healthy pregnant women increased by 23.9%, parameters of frontal occipital head size by 21.6%, head circumference by 34.8%. These indicators in fetuses of pregnant women in a state of hypothyroidism had similar values to those in fetuses of healthy pregnant women, the biparietal diameter increased by 26.9%, the frontal-occipital size by 24.3%, the head circumference by 26.4%.In the periods between the second and third screening examinations (26-30 weeks), the intensity of the growth of the head size in fetuses increased more intensively in pregnant fetuses in a state of hypothyroidism. Analysis of the data shows that the rate of increase in biparietal head diameteres in fetuses of healthy pregnant women was 18.7%, frontal occipital size - by 23.6%, head circumference - by 14.8%. In fetuses of pregnant women in a state of hypothyroidism, these indicators were 19.4%, 17.7%, 21.3%.The smallest growth rate of fetometry indicators was noted during the third screening examination. The biparietal diameter in fetuses of healthy pregnant women increased by 3.1%, the frontal occipital size - by 5.7%, and the head circumference - by 14.8%. In fetuses of pregnant women in a state of hypothyroidism, these indicators were 3.4%; 7% vs. 16%.The growth rate of fetometry values in 12 to 35 weeks in fetuses of healthy pregnant women increased biparietal head diameter by 292.7%, frontal occipital size by 297.8%, and head circumference by 313.7%.In fetuses of pregnant women in a state of hypothyroidism, during the studied period, the growth rate of head parameters increased biparietal diameter by 296%, frontal occipital size - by 295.6%, head circumference - by 302.8%.
4. Conclusions
Thus, it can be concluded that the results obtained using the in vivo method of research on the peculiarities of the development of the cerebral skull in fetuses complement and develop research on craniology, including in the age aspect at the stage of prenatal ontogenesis under normal and pathological conditions. In fetuses of pregnant women with hypothyroidism, the bipariteal and frontal-occipital head sizes were significantly smaller at the stage of the second screening examination than in fetuses of healthy pregnant women. The circumference of the head of fetuses of pregnant women in a state of hypothyroidism at all stages is less than that of fetuses of healthy pregnant women. In general, during the entire observation period, there was an equal rate of growth of the biparietal size and the predominant intensity of growth of the frontal-occipital size and head circumference in pregnant fetuses in the state of hypothyroidism. In fetuses of pregnant women with hypothyroidism, the biparietal and frontal - occipital head sizes were significantly (p<0.05) smaller at the stage of the second screening examination than in fetuses of healthy pregnant women. The circumference of the head of fetuses in pregnant women in a state of hypothyroidism at all stages is less than in the fetuses of healthy pregnant women, but from the point of view of statistics, this hypothesis has not been proven.
References
| [1] | Zaydiyeva Z. S., Yakunina N. A., Prozorov V. V. Lecheniye i profilaktika defitsita yoda vo vremya beremennosti // Russkiy meditsinskiy jurnal. 2008. T. 16, № 19. 329 s. |
| [2] | Kiyenya T.A., Morgunova T.B., Fadeyev V.V. Vtorichnyy gipotireoz u vzroslykh: diagnostika i lecheniye // Klinicheskaya i eksperimental'naya tireoidologiya. -2019 –T.15 – N.2 – S. 64 – 72. |
| [3] | De Groot L., Abalovich M., Alexander E.K., Amino N., Barbour L. et al. Management of Thyroid Dysfunction during Pregnancy and Postpartum: An. Endocrine Society. Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2012; 97 (8): 2543–2565. |
| [4] | Glinoer D. Thyroid immunity, thyroid dysfunction, and the risk of miscarriage (Editorial) // Amer J. Reprod. Immunol. 2000. — V. 43.— P. 202. |
| [5] | Koulouri O, Auldin MA, Agarwal R et al. Diagnosis and treatment of hypothyroidism in TSH deficiency compared to primary thyroid disease: pituitary patients are at risk of underreplacement with levothyroxine. Clin Endocrinol 2011; 74: 744–749. |
| [6] | Krassas G. E., Poppe K., Glinoer D. Thyroid function and human reproductive health. Endocr. Rev. 2010. — 31.— P. 702–755. |
| [7] | Leger J, Olivieri A, Donaldson M et al. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. Horm Res Paediatr 2014; 81: 80–103. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML