Kurbonov Sh. Zh.1, Amonov Sh. E.2, Bakieva Sh. Kh.2
1Tashkent Pediatric Medical Institute, Uzbekistan
2Tashkent Medical Academy, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article provides a comparative characteristic of surgical methods for the treatment of chronic inflammatory diseases of the maxillary sinus. The comparison groups consisted of patients with various productive diseases of the maxillary sinus at the age of 18-65 years who were hospitalized at the clinic of the Tashkent Pediatric Medical Institute in 2017-2019. The results of the study showed that the most effective method of surgical intervention is endonasal access through the lower nasal passage, followed by plasty of the medial wall of the maxillary sinus. Opening of the maxillary sinus through the lower nasal passage can be classified as functional surgery, since this type of intervention does not affect the intact structures of the osteomeatal complex.
Keywords:
Endoscopic surgery, Maxillary sinus, Plastics of the medial wall of the maxillary sinus, Uncinate process
Cite this paper: Kurbonov Sh. Zh., Amonov Sh. E., Bakieva Sh. Kh., Comparative Evaluation of the Results of Different Surgical Interventions in Patients with Chronic Inflammatory Diseases of the Maxillary Sinus, American Journal of Medicine and Medical Sciences, Vol. 11 No. 4, 2021, pp. 268-270. doi: 10.5923/j.ajmms.20211104.02.
1. Introduction
The choice of the optimal access for surgical intervention in the maxillary sinus (MS) remains an urgent problem [2,6,7]. Choosing this or that approach, the surgeon should be guided by the type of pathology, anatomical accessibility and physiological permissibility of the method, and only last but not least by his personal preferences [1,4].To date, there is no universal access to MS. This is evidenced by the lack of satisfaction with the existing methods and the constant search for new methods. Based on the surgical pathology of MS, for its successful treatment, it is necessary to carry out adequate sanitation, removal of pathological contents, as well as revision of the natural anastomosis. Important is the possibility of manipulation in the lower parts of the sinus, as well as the high physiology of the proposed method [3,5,9].Opening of the maxillary sinus (MS) is one of the most common surgical procedures in rhinosurgery. There are several surgical approaches to MS. Distinguish between external and intranasal accesses. It was noted that external variants of approaches to the MS are often accompanied by reactive edema of the soft tissues of the face, prolonged paresthesia and neuralgia of the branches of the trigeminal nerve, as well as a relatively long recovery period. In recent years, external access interventions on the paranasal sinuses (PNS) have significantly decreased. Currently, access through the anterior or lateral walls of the sinus, the socket of the tooth is used more in dental and oncological practice. The introduction of microscopic and endoscopic techniques has expanded the possibilities of intranasal surgery. There is a trend towards endonasal endoscopic surgery, which, being less traumatic, can provide adequate debridement of chronic foci of infection with PNS and MS in particular [2,10].Endonasal dissection of the MS can be performed in different ways: through the middle (MNP) and lower (LNP) nasal passages. The most common access to the MS today is the method of expanding its natural anastomosis. However, this method, as a rule, implies a violation of the architectonics of the ostiomeatal complex (OMC), which is not always justified in the normal functioning of the natural anastomosis. In addition, this approach creates technical difficulties in the localization of the pathological process in the area of the lower and anterior sections of the MS. The formation of a persistent anastomosis of the MS with the nasal cavity in the LNP area is also not required if there is no need to increase sinus ventilation [4,7].In recent years, the indications for MS sanitation have expanded (dental implantation, sinus lifting, sanitation of foci of chronic infection before organ and tissue transplantation, issues of professional suitability, etc.), it became necessary to develop a minimally invasive endoscopic approach to MS, allowing to preserve normally functioning structures of OMC [8,9].The aim of this study was to compare the results of various surgical interventions in patients with chronic inflammatory diseases of the maxillary sinus.
2. Materials and Methods
The study material was composed of patients with various productive diseases of the maxillary sinus at the age of 18-65 years, who were hospitalized at the clinic of the Tashkent Pediatric Medical Institute in 2017-2019. The study group included 55 men (55%) and 45 women (45%) aged 18 to 76 years. The average age of the patients was 48 years. The criteria for the formation of clinical groups were the presence of productive forms of chronic sinusitis (cyst, polyp) and the need (justification) of surgical treatment, as well as the absence of acute respiratory diseases at the time of examination and a history of allergic diseases. In the general structure of endoscopic surgical interventions on the maxillary sinus, the following types of sinus lesions can be distinguished: 22% - chronic polyposis rhinosinusitis, 35% - cysts of the maxillary sinuses, 31% - foreign bodies of the maxillary sinuses, 8% - chronic maxillary sinusitis, 4% - chronic maxillary ethmoiditis. We used 2 options for opening the affected maxillary sinuses: through the canine fossa (micromaxillotomy), lower nasal passage.All patients underwent a comprehensive clinical and laboratory examination, including collection of anamnesis of the disease, rhinoendoscopy, morphological and computed tomographic examination. Statistical data processing was performed using the Microsoft Excel 2016 and Statistics 8 software package.
3. Research Results and Their Discussion
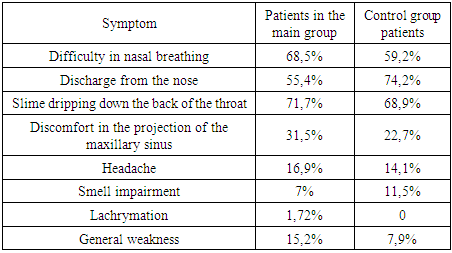
When assessing patients' complaints before surgical treatment, the leading symptom was mucus / discharge along the posterior pharyngeal wall or postnasal rhinorrhea. In 70,9% cases noted the presence of this complaint. 63,6% cases complained of nasal discharge. Headache and facial pain were reported by 15,5% patients. 27,2% patients noted discomfort in the projection of the maxillary sinus. Lacrimation was detected in 0,9% patient. 12% of cases had no complaints from the ENT organs (Table 1).Table 1. The structure of patient complaints before surgical treatment
 |
| |
|
During the preoperative examination, all patients underwent computed tomography using a cone-beam tomograph. Unilateral lesion of the maxillary sinus was revealed in 86,23% cases, surgical treatment for MS was performed on one side, in 13,77% cases - on two sides. The spectrum of the revealed pathology of the maxillary sinus included cyst-like formations, foreign bodies (teeth and their fragments, filling material, implants). The pathological process in most cases in all examined groups was located in the basal sections of the sinus.Cyst-like formations of the maxillary sinus were found in 60% cases. The vast majority of cysts were localized in the region of the lower wall of the sinus (35,9%) cases) or occupied the entire volume of the sinus (52,4%) cases). A rare localization of the cyst on the orbital wall of the upper junction in the projection of the II branch of the trigeminal nerve was noted in 1,28% case.Foreign bodies were also visualized in the area of the bottom and alveolar bay (60%) and, in a small percentage of cases, in the projection of the anterior (14,1%) cases) and medial (17,5%) walls).Bullous changed middle turbinate was detected in 8,6% cases. In 44,44% cases, an air cell was found in the right middle turbinate, in 22,22% cases - in the left and in 33,33% cases - bilateral “concha bullosa”. In 1,8% patients, aplasia was revealed, in 2,72% - hypoplasia of the frontal sinuses with preserved pneumatization of the remaining sinuses. Curvature of the nasal septum was detected in 37,3% cases.The patients of the main group used the technique of opening the maxillary sinus through the lower nasal passage. Local anesthesia was performed under general anesthesia for isolated lesions of the maxillary sinuses. The inferior turbinate is displaced medially and the location of the lacrimal canal outlet is assessed by pressing on the lacrimal sac region in the medial corner of the eye. Then, outside the zone of the lacrimal canal, the lateral wall of the nasal cavity is perforated simultaneously through all layers with a raspor from the attachment point of the inferior turbinate to the bottom of the nasal cavity with a length of 1-1.5 cm, the resulting flap is pushed back and medially. A gap is formed through which pathological contents are removed from the sinus cavity under the control of an endoscope. The superimposed anastomosis was closed, depending on the nature of the pathological process. In case of closure of the anastomosis, the flap of the lateral wall of the nasal cavity is put in place, the sheets of the mucous membrane are compared with the help of a raspator, and the inferior turbinate is returned to its natural position.Observations of patients showed that when performing plastic surgery of the anastomosis in the lower nasal passage, after 2 months at the site of surgery, gentle cicatricial changes are visualized, sometimes comparable to puncture marks that do not violate the anatomical integrity of the sinus.When conducting a questionnaire after the operation on the 5th day, an increase in nasal congestion and discharge from the nose was noted. The nature of the discharge in postoperative patients acquired a muco-hemorrhagic character, no purulent discharge was noted. Patients did not notice discomfort in the sinus projection, and in the case of its initial presence, it regressed 1-5 days after the intervention. 6 months after the operation, regression of symptoms was noted in all groups.The results of PARM in dynamics indicate a decrease in edema of the mucous membrane, a subsidence of inflammation in the area of surgical treatment and restoration of the air flow rate in a short time. According to the results of the study, no significant effect of the pathological process in the MS and surgical access to the sinus on nasal breathing was revealed.Among all the operated patients, no serious complications were noted in any patient. In 3,5% patients in group I and in 5,6% patients in group II, nosebleeds were observed in the postoperative period against the background of increased blood pressure. After the appointment of antihypertensive therapy and systemic hemostatic therapy, nosebleeds were stopped. Damage to the II branch of the trigeminal nerve was not observed in any of the cases. There were also no cases of damage to the orbit and nasolacrimal canal.During the dynamic examination of patients in the postoperative period a relapse of the disease was detected in 1,5% cases: 1,5% cysts and 2% foreign bodies. All patients were successfully reoperated.The methods of surgical treatment of the pathology of the maxillary sinus have been known for several centuries and continue to develop and improve. This is due to the high prevalence of changes in the maxillary sinus and the availability of anatomical and topographic location. However, there is currently no uniform approach to surgery. The trend towards minimally invasiveness has left its mark on the methods of opening the maxillary sinus. More and more attention is paid to the preservation of normally functioning nearby anatomical structures. The original opinion within the FESS that it is physiologically possible to operate the sinus only through the natural anastomosis is currently undergoing changes. The expansion of the natural anastomosis has its limitations. Expressed aeration of the paranasal sinuses leads to a change in their gas composition, which can in itself trigger a cascade of pathological reactions. Therefore, while maintaining the normal architectonics of the ostiomeatal complex, it is necessary to strive to preserve its anatomy.Increasing attention is being paid to the lower nasal passage, an area that lacks large blood vessels and nerves and is far from the eye socket and brain.A feature of interventions through the lower nasal passage is that they carry the potential danger of damage to the lacrimal passages. But the development of endoscopic equipment makes it possible to identify the outlet of the lacrimal duct and, thus, reduce the risk of damage.Operational techniques that involve closing the temporary surgical access meet the requirements of functional sinus surgery. Since the intervention ends with the restoration of the integrity of the sinus.Thus, it follows that the operation using the access through the lower nasal passage can be offered as a teaching component. Since the risks to the patient with this type of intervention are minimal.
References
| [1] | Ashman A. et al. Extended endoscopic approaches to the maxillary sinus // The Journal of Laryngology & Otology. – 2020. – Т. 134. – №. 6. – С. 473-480. |
| [2] | Fokkens W. J. European position paper on rhinosinusitis and nasal polyps 2020 //Rhinology. – 2020. – Т. 58. – №. Supplement 29. – С. 1-464. |
| [3] | Hong W. et al. Development of a novel continuum robotic system for maxillary sinus surgery // IEEE / ASME Transactions on Mechatronics. – 2018. – Т. 23. – №. 3. – С. 1226-1237. |
| [4] | Kryukov A. I. et al. The strategy of the of surgical treatment of the cysts in the maxillary sinus //Vestnik otorinolaringologii. – 2019. – Т. 84. – №. 1. – С. 42-45. |
| [5] | Levine C. G., Casiano R. R. Revision functional endoscopic sinus surgery //Otolaryngologic Clinics of North America. – 2017. – Т. 50. – №. 1. – С. 143-164. |
| [6] | Naros A. Fungus ball of the maxillary sinus—modern treatment by osteoplastic approach and functional endoscopic sinus surgery // Journal of Oral and Maxillofacial Surgery. – 2019. – Т. 77. – №. 3. – С. 546-554. |
| [7] | Nomura K. et al. Endoscopic modified medial maxillectomy for fungal ball of the hypoplastic maxillary sinus with bony hypertrophy // Journal of Craniofacial Surgery. – 2018. – Т. 29. – №. 3. – С. e304-e307. |
| [8] | Philpott C., Sama A. Endonasal Approaches to Maxillary Sinus // International Journal of Head and Neck Surgery. – 2018. – Т. 9. – №. 1. – С. 26-31. |
| [9] | Siu J. et al. Quantification of airflow in the sinuses following functional endoscopic sinus surgery //Rhinology. – 2020. – Т. 58. – №. 3. – С. 257-265. |
| [10] | Zhao Y. et al. Modified endoscopic inferior meatal fenestration with mucosal flap for maxillary sinus diseases // Videosurgery and Other Miniinvasive Techniques. – 2018. – Т. 13. – №. 4. – С. 533. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML