-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(3): 240-245
doi:10.5923/j.ajmms.20211103.17
Received: Feb. 27, 2021; Accepted: Mar. 22, 2021; Published: Mar. 28, 2021

Influence of Chlamydia Infection Associated with Rheumatoid Arthritis on the Activity of the Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDilrabo Abdurazzakova1, Seytbay Matchanov1, Nikolai Soroka2
1Tashkent Medical Academy, Uzbekistan
2Belarusian State Medical University, Belarus
Correspondence to: Seytbay Matchanov, Tashkent Medical Academy, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

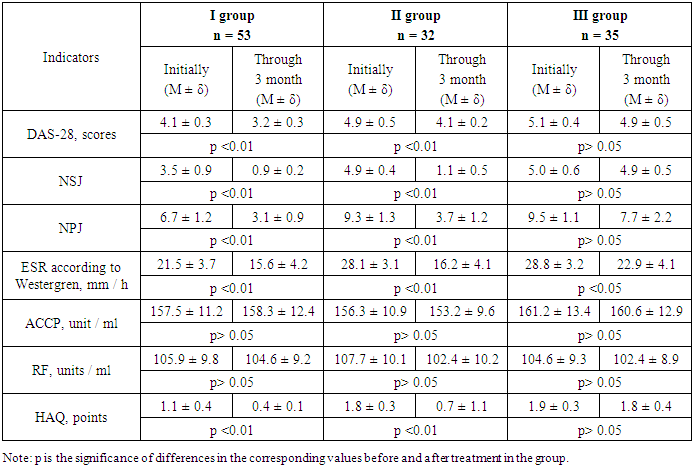
Many factors affect the course of rheumatoid arthritis (RA), including infection. In the study of synovial fluid in patients with RA by polymerase chain reaction (PCR), a higher incidence of Chlamydia trachomatis infection (C. trachomatis) was found in comparison with the control group. The aim of the study was to evaluate the effect of chlamydial infection associated with RA on disease activity. 120 patients with RA were examined. The study included patients with RA who met the classification criteria of the American College of Rheumatology / European Anti-Rheumatic League (ACR / EULAR, 2010), who were hospitalized in the multidisciplinary clinic of the Tashkent Medical Academy. Patients were divided into 3 groups: group I - 53 patients with RA, II - 32 patients with RA in combination with chlamydial infection treated with chlamydial infection, Group III - 35 patients with RA combined with chlamydial infection who did not eradicate chlamydial infection. For all examined RA patients, methotrexate at a dose of 20 mg / week was prescribed as basic therapy. A re-evaluation of the effectiveness of treatment in patients with RA was carried out after 3 months.The results of the studies showed that indicators such as the Disease Activity Score (DAS-28), the number of swollen joints (NPV), the number of painful joints (CHS), the erythrocyte sedimentation rate (ESR), and the health assessment indicators Questionnaire (HAQ), the vitality and mental health of patients in group I were significantly lower than similar indicators of groups II and III of patients. This may indicate that when RA is combined with chlamydial infection, the activity of the disease is higher than with RA without chlamydial infection. In the first group, basic therapy with methotrexate 20 mg / week for three months had a positive effect on RA activity indices. In the treatment dynamics, such indicators as DAS-28, (p <0.01), NPV (p <0.01), CHB, (p <0.01), ESR, (p <0.01) differed significantly in the dynamics of treatment. , HAQ, (p <0.01). In the II group, after the eradication of chlamydial infection, positive dynamics of DAS-28, (p <0.01), NPV (p <0.01), ChBS, (p <0.01), ESR, (p <0, 01), HAQ, (p <0.01). At the same time, in group III, where patients with RA did not undergo eradication of chlamydial infection, only ESR significantly decreased (p <0.05).The study showed that the presence of chlamydial infection in patients with RA is associated with an increase in the activity of the pathological process. When managing patients with chlamydial infection, the recommended treatment goal is much less often achieved - remission or low disease activity. The presence of chlamydial infection in patients with RA requires the eradication of chlamydial infection, which helps to improve the general condition of patients, has a favorable effect on the course of the underlying disease before prescribing basic anti-inflammatory therapy.
Keywords: Rheumatoid arthritis, Basic therapy, Chlamydial infection, Disease activity
Cite this paper: Dilrabo Abdurazzakova, Seytbay Matchanov, Nikolai Soroka, Influence of Chlamydia Infection Associated with Rheumatoid Arthritis on the Activity of the Disease, American Journal of Medicine and Medical Sciences, Vol. 11 No. 3, 2021, pp. 240-245. doi: 10.5923/j.ajmms.20211103.17.
1. Introduction
- Rheumatoid arthritis (RA) is an immuno-inflammatory (autoimmune) rheumatic disease of unknown etiology, characterized by chronic erosive arthritis and systemic damage to internal organs, leading to early disability and shortening the life expectancy of patients [1]. The development of RA is determined by the complex interaction of environmental factors and a genetic predisposition leading to global disturbances in the system of humoral and cellular immunity [2,3]. RA is a frequent and one of the most severe immuno-inflammatory diseases in humans, which determines the great medical and socio-economic importance of this pathology. The prevalence of RA among adults in different geographical areas of the world ranges from 0.5 to 2%. The ratio of women to men is 4: 1. The disease occurs in all age groups, but the peak incidence occurs at the most working age - 40-55 years. RA causes a permanent loss of disability in half of patients during the first 3-5 years from the onset of the disease and leads to a significant reduction in their life expectancy due to the high incidence of cardiovascular pathology, severe infections, cancer, and the complications associated with RA systemic immuno-inflammatory process [1].RA, like most other autoimmune and inflammatory processes, has a multifactorial nature: 30-60% of the risk of its development is due to a genetic predisposition, 40-70% is associated with the influence of environmental factors [4]. The evolution of RA includes several successively (or discretely) developing stages. There are “preclinical” stages that are transformed into “symptomatic”, ending with the formation of a clinical and laboratory symptom complex characteristic of early and then advanced RA [5,6]. The nature of the interaction of environmental factors, genetic predisposition and immune mechanisms that determine the transition from stage to stage, progression options, the nature and severity of extra-articular (systemic) manifestations and the risk of comorbid diseases are not completely clear and are currently the subject of intensive research [2].In recent years, with the accumulation of data obtained within the framework of national registers and observational studies, the problem of combined pathologies has been of increasing interest [7]. Often, patients with RA do not receive sufficient treatment for concomitant diseases, and multimorbid pathology can adversely affect the activity of RA [8]. At the same time, the appointment of genetic engineering biological drugs (GBI) in these patients is often postponed, despite the available indications for their appointment [9]. Inadequate treatment of RA, in turn, can contribute to the progression of concomitant pathology, while active treatment of rheumatic diseases (RH) can ensure its positive dynamics [10,11]. It should be noted that the recommendations for treatment “treat to target” [12] are based on data that were obtained in clinical trials involving patients without significant concomitant disorders, therefore, the effect of associated conditions was not taken into account. In our opinion, this greatly limits the possibility of using the available recommendations in real clinical practice, when doctors have to manage patients with concomitant diseases. Further studies are needed to evaluate the possibilities of modern antirheumatic therapy in patients with concomitant diseases.The need for a detailed assessment of the effects of concomitant pathology on the course of RA is due to the fact that, despite new methods for early diagnosis of the disease, scientifically based treatment strategies, including using high-tech methods, it is far from always possible to achieve a pronounced improvement in the condition of the patient as a whole, to maintain its functional activity and, thereby, significantly optimize the long-term prognosis [7,13,14].The course of RA is affected by many factors, including infection. In the study of synovial fluid in patients with RA by PCR, a higher incidence of Chlamydia trachomatis infection (C. trachomatis) was found in comparison with the control group [15,16,17]. This infection belongs to the family Chlamydiacea. The latter combines C. psittaci, C. pneumoniae, and C. trachomatis. The genus Chlamydia is C. trachomatis, which was first isolated from the urogenital tract of B. Jones in 1949. C. trachomatis is the most common sexually transmitted infection [12]. The role of chlamydia in the etiopathogenesis of articular and rheumatic diseases is largely due to the molecular similarity of their antigens with autoantigens of the macroorganism [18].Most people with C. trachomatis infection are unaware of the presence of a chronic infection in the body because they do not have symptoms that prompt them to seek medical help [19]. However, the persistence of C. trachomatis in RA affects the rate of development of destructive changes in the joints [20,21], and the RA associated with chlamydial infection has its own clinical and radiological features and is a peculiar variant of the course of RA [22].The influence of C. trachomatis on the course of RA and the nature of the musculoskeletal system lesion should be taken into account when choosing treatment tactics. If a chlamydial infection is detected in the urogenital tract or synovial fluid of patients with RA, etiotropic therapy is necessary, ideally before eradication of the infection. Recent studies have established the fact that in some patients with RA, in association with chlamydial infection, against the background of basic anti-inflammatory therapy, a hyperthermic reaction is clearly observed [23]. At the same time, after a course of antibiotic therapy, body temperature is normalized, which indicates that the presence of chlamydial infection in patients with RA worsens the clinical course of the underlying disease. At the same time, in the literature insufficient attention is paid to the problem of “cohabitation” of the RA and chlamydial infection. Currently, there are very few publications on RA associated with chlamydial infection [24].The presence of chlamydial infection in the body of patients with RA complicates the course of the articular syndrome, affects the activity of the underlying disease.The aim of the study was to evaluate the effect of chlamydial infection associated with RA on disease activity.
2. Patients and Methods
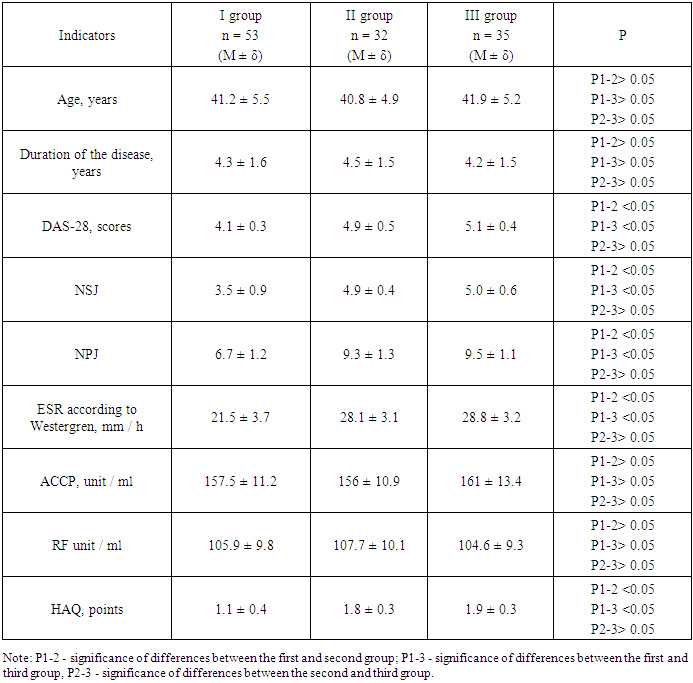
- 120 patients with RA were examined. The study included patients with RA that meet the classification criteria of the American College of Rheumatology / European Anti-Rheumatic League (ACR / EULAR, 2010) [25], who were hospitalized in the multidisciplinary clinic of the Tashkent Medical Academy. Patients were divided into 3 groups: group I - 53 patients with RA, II - 32 patients with RA in combination with chlamydial infection treated with chlamydial infection, Group III - 35 patients with RA combined with chlamydial infection who did not eradicate chlamydial infection. For all examined RA patients, methotrexate at a dose of 20 mg / week was prescribed as basic therapy. A re-evaluation of the effectiveness of treatment in patients with RA was carried out after 3 months.The duration of the disease at the time of the initial examination ranged from 1 year to 7 years (on average in the first group 4.3 ± 1.6 years, in the second group 4.5 ± 1.5 years, in the third group 4.2 ± 1.5 years old); the average age of patients in group I was 41.2 ± 5.5 years, in group II - 40.8 ± 4.9 years, in group III - 41.9 ± 5.2 years. Most patients of group I (45 patients - 84.9%), 27 patients (84.3%) of group II and 30 patients (85.7%) of group III with RA are seropositive for rheumatoid factor (RF), antibodies to cyclic citrulinated peptide (ACCP) were detected in 41 patients (77.3%) of group I, in 25 patients (78.1%) - of group II, and in 27 patients (77.1%) - of group III.Statistical processing was performed using the Statistica program, version 10.0 (StatSoft). To describe the quantitative data, mean (M) with standard deviation (δ). Comparison of groups was carried out using Student's t-test. Differences were considered statistically significant at p <0.05.
3. Results and Discussion
- The results of the studies showed that such indicators as age, duration of the disease, ADCP and RF did not statistically differ in the observation groups (p> 0.05), (table 1). Other indicators, like Disease Activity Score (DAS-28), number of swollen joints (NPV), number of painful joints (CHS), erythrocyte sedimentation rate (ESR), Health Assessment Questionnaire (HAQ), vitality and mental health of patients in group I were significantly lower than similar indicators of groups II and III of patients. This may indicate that when RA is combined with chlamydial infection, the activity of the disease is higher than with RA without chlamydial infection.
|
|
4. Conclusions
- The study showed that the presence of chlamydial infection in patients with RA is associated with an increase in the activity of the pathological process. When managing patients with chlamydial infection, the recommended treatment goal is much less often achieved - remission or low disease activity. The presence of chlamydial infection in patients with RA requires the eradication of chlamydial infection, which helps to improve the general condition of patients, has a favorable effect on the course of the underlying disease before prescribing basic anti-inflammatory therapy.