-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(3): 189-192
doi:10.5923/j.ajmms.20211103.06
Received: Jan. 31, 2021; Accepted: Feb. 22, 2021; Published: Mar. 15, 2021

Morphological Justification of Organ-Preserving Operations in Obstetric Practice
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUmarova Nargiza Mirzaevna1, Tursunov Khasan Ziyaevich2, Ayupova Farida Mirzaevna3, Nigmatova Gulnora Maksudovna3
1Deputy Director of the Republican Perinatal Center, Tashkent, Uzbekistan
2Department of Pathological Anatomy, Tashkent Medical Academy, Tashkent, Uzbekistan
3Department of Obstetrics and Gynecology, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Umarova Nargiza Mirzaevna, Deputy Director of the Republican Perinatal Center, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article provides data on the results of histological studies of tissues excised from a scar or surgical wound in 30 puerperas at different times after Caesarean section (CS) with inconsistency of the suture on the uterus, complicated by septic metroendometritis, obstetric peritonitis. Conducted morphological studies substantiate the local invasive organ-preserving operation - the imposition of secondary sutures (ISS), and confirm the presence of an inflammatory process, since despite the ongoing reparation processes in the myometrium, the picture of endometrial inflammation persists. In the long-term follow-up (after 12-16 days), the repair and remodeling of tissues in the myometrium increased. Along with the proliferation of fibroblasts and fibrocytes, the proliferation of fibrous tissue is noted not only in the interstitium, but also around the vessels with thickening of their walls, symptoms of vasculitis. Carrying out ultrasound and doplerometric studies in the postoperative period, in order to study involutive processes in the uterus, contributes to the early detection of inflammatory postoperative complications and the timely prevention of generalization of postoperative purulent-septic diseases after CS, as well as to assess the effectiveness of the therapy of these complications during the healing process, postoperative wound repair.
Keywords: Pregnancy, Caesarean section, Suture failure, Metroendometritis, Sepsis, Morphology, Fibrosis
Cite this paper: Umarova Nargiza Mirzaevna, Tursunov Khasan Ziyaevich, Ayupova Farida Mirzaevna, Nigmatova Gulnora Maksudovna, Morphological Justification of Organ-Preserving Operations in Obstetric Practice, American Journal of Medicine and Medical Sciences, Vol. 11 No. 3, 2021, pp. 189-192. doi: 10.5923/j.ajmms.20211103.06.
Article Outline
1. Introduction
- The problem of postoperative complications in obstetric practice is still an urgent problem in modern healthcare. Surgical interventions during childbirth and the postpartum period are increasing every year [1,4]. Postoperative complications in the early period are associated with inconsistency of scars or the addition of infection with the development of inflammation, and in the late postpartum period - the formation of adhesions. The latter affect subsequent childbirth and again lead to surgical interventions [5]. One of the main reasons for the development of inconsistency of sutures and postoperative scar on the uterus is inflammation with the development of metroendometritis [2,5]. According to the results of the III confidential analysis of maternal mortality cases for 2016 - 2017. (KSMIS) "In the name of saving the mother's life", the cause of maternal mortality from sepsis was 3%, and according to various authors, the incidence of purulent-septic complications of the postpartum period varies from 1 - 54.38% [1,4,5]. Postpartum endometritis is the most common complication of a caesarean section [5], and the risk of its development after surgery is 5-10 times higher than after natural childbirth. Development of postpartum endometritis, the more complicated by sepsis, in normal practice, the uterus is amputated and at the same time leaving the woman infertile in the future. Postoperative wound healing is a complex process that includes inflammation, angiogenesis, tissue formation and remodeling [4,5].As can be seen from our practice, there are primiparous patients in whom childbirth ended in stillbirth (62.5%) and was complicated by sepsis, obstetric peritonitis, the source of which was the uterus. In this connection, we have been using organ-preserving tactics for the management of postpartum septic complications in the ROC since 2016, thereby giving a chance for the subsequent preservation of reproductive function in young women. However, one should resort to the preservation of the genital organ only in cases where the reserve forces of the woman's body allow the preservation of the uterus, for which we develop an algorithm and criteria for the management of such patients, which is confirmed by the morphological picture, immunological studies, and methods of functional diagnostics.
2. The Purpose of the Research
- The aim of the study was to substantiate organ-preserving operations after cesarean section (CS) with inconsistency of the suture on the uterus, complicated by septic metroendometritis, obstetric peritonitis based on the study of morphological aspects.
3. Materials and Methods
- The material for the study was the surgical material - excised from a scar or surgical wound in 30 puerperas at different times after a Caesarean section (CS). In the postoperative period, complications were observed in the form of metroendometritis, peritonitis, abscesses of the small pelvis, sepsis and septic shock. Women were divided into groups according to the time of admission after ACS: group 1: up to 3 days (1 w.); Group 2: 4 -7th day (6 days); 3- group: 8-15 days (12 days); 4- group: 16-24 days (5 days); 5- group: more than 25 days (6 cases) After the repeated operation, the state of the sutures on the uterus and the healing of the surgical wound were monitored by ultrasound [3]. A general morphological research method was used - staining the sections with hematoxylin and eosin. The preparations were prepared according to the generally accepted technique: fixation of the material in a 10% solution of neutral formalin, dehydration in alcohols of increasing concentration, embedding in paraffin, cutting on an MC-2 microtome, and staining of sections 4-5 μm thick with hematoxylin and eosin. Photo-graphing of micropreparations was carried out on a DN-300M microscope.
4. Results
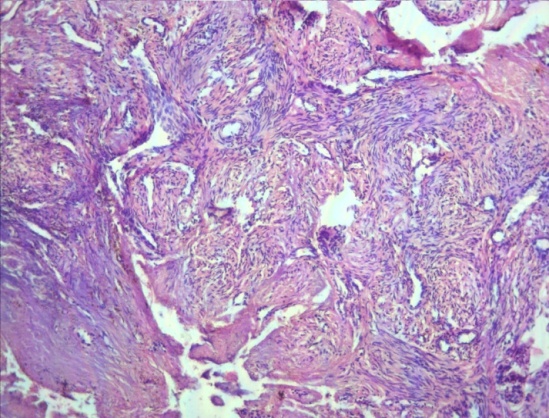
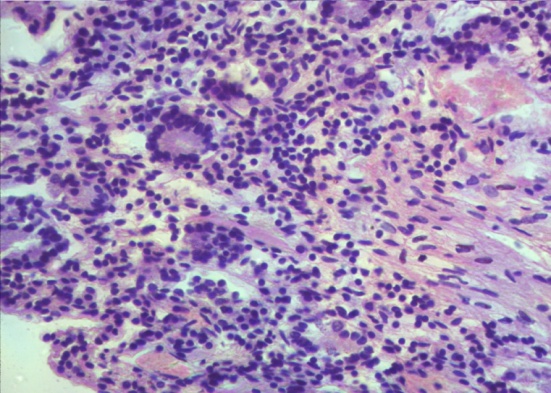
- The number of stillborns - 16 (51.6%) and live births - 15 (48.3%) newborns in puerperas who underwent organ-preserving surgery after CS and the number of dead-borns in primary pregnant women from all cases of stillbirth is 16 (62.5%).In the early (1-3 days) after CS, diffuse purulent inflammatory infiltration of the myometrium was observed in the area of the surgical wound, muscle fibers were fused, their structure was not determined (Fig. 1). After 3 days after CS, purulent fusion of tissues with necrosis was accompanied by hemorrhage and hemorrhagic infiltration (Fig. 2). In the future, inflammatory infiltration also underwent necrosis, tissue melting with complete disruption of the structure, thrombosis in the vessels of the microcirculatory bed were noted (3). Inflammatory infiltration was also observed in the endometrium, where the glands were partially destroyed, in the lumen of their desquamated epithelium and leukocytes. In places the glands are compressed, reduced in size, some are destroyed, hemorrhages are noted (Fig. 4).
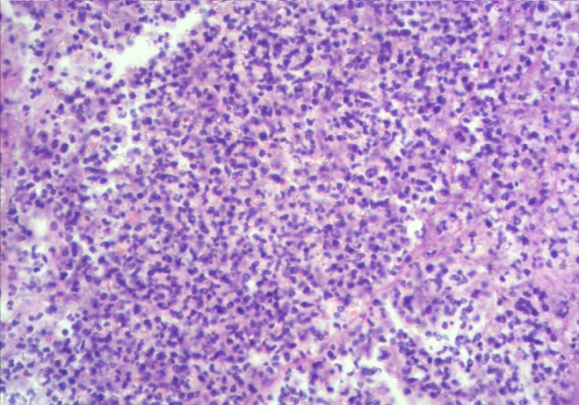 | Figure 1. Diffuse inflammatory purulent infiltration of the myometrium with necrosis. Staining with hematoxylin and eosin. 10x4 |
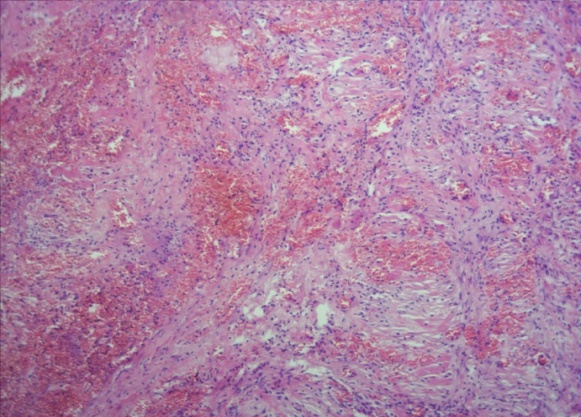 | Figure 2. Diffuse inflammatory infiltration, edema, plethora of capillaries with hemorrhages with imbibition. Staining with hematoxylin and eosin. 10x10 |
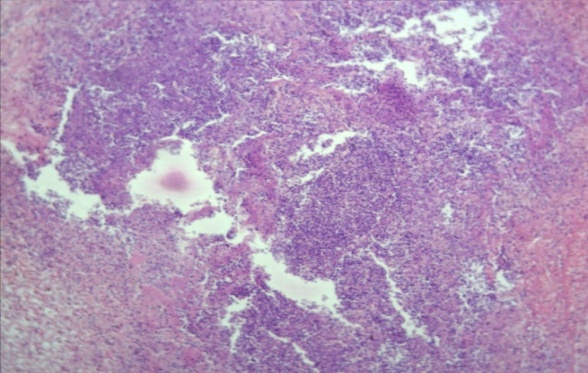 | Figure 3. Necrosis of tissue and infiltration (abscess formation). Staining with hematoxylin and eosin. 10x10 |
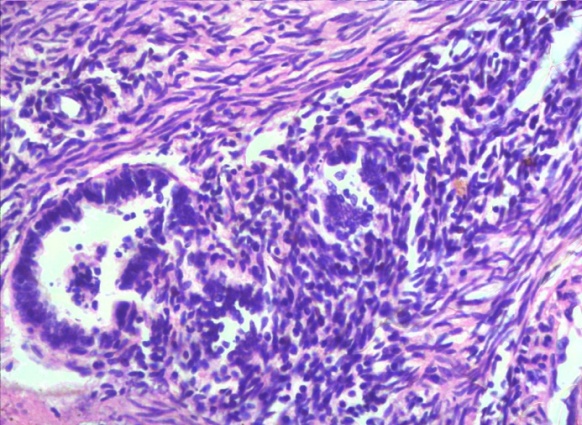 | Figure 4. Metroendometritis. Inflammatory infiltration of the endometrium with destruction of glands and proliferation of connective tissue. Staining with hematoxylin and eosin. 10x40 |
 | Figure 5. Overgrowth of connective tissue, many capillaries. Staining with hematoxylin and eosin. 10x40 |
 | Figure 6. The endometrium is edematous, with fibrin deposition and inflammatory infiltration. Staining with hematoxylin and eosin. 10x10 |
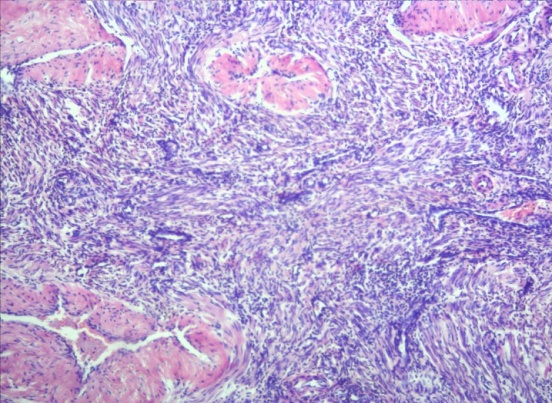 | Figure 7. Overgrowth of cellular and fibrous connective tissue in the myometrium. Staining with hematoxylin and eosin. 10x40 |
5. Conclusions
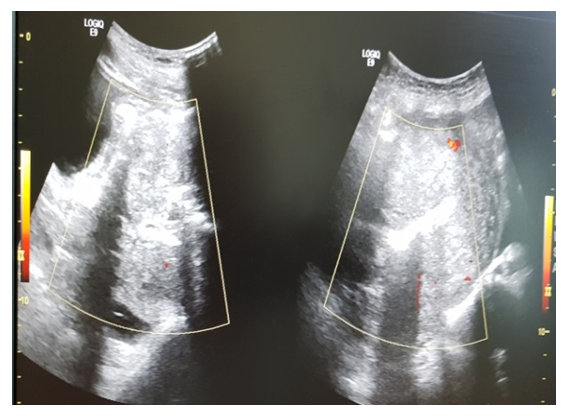
- The studies carried out indicate the development of metroendometritis at different times of the ACS. In the early stages (3-7 days), inflammatory and destructive changes in endomyometrium prevail. In the subsequent periods, reparative processes predominate, hemorrhages, necrotic detritus resolve, cellular and fibrous tissue grows against the background of inflammation, adhesions are formed.Healing of a postoperative wound is a complex process, the morphological picture of which consists of polymorphic inflammatory infiltration of the myometrium with hypertrophy of stromal-parenchymal elements, including: inflammation, angiogenesis, formation and remodeling of tissues, with the formation of an adhesive process, and symptoms of vasculitis.After excision of necrotic-inflammatory tissues in the uterus, the healing is monitored by ultrasound and dopplerometry is performed in dynamics: visualization of the healing of secondary sutures on the uterus, the structure and vascularization in the myometrium and the area of the surgical scar, measurement of blood flow in the uterus.Inconsistency of the suture on the uterus (ISU) Spox 10 days - sepsis, obstetric peritonitis. Before and after organ-preserving surgery - the imposition of secondary sutures on the uterus.Echographic assessment of the state of the suture on the uterus in a third of women with endometritis revealed hematomas (usually small) under the vesicouterine fold. In 42.9% of women with endometritis, the inflammatory process involved the myometrium in the suture area. In 23.8% of patients, echographic signs of an inflammatory process in the myometrium were combined with the manifestation of its anatomical inconsistency, which was expressed in the formation of a wall defect from the side of the uterine cavity due to a niche of an irregular triangular shape and a pronounced thinning of its distal part (Fig. 8) -one). In our opinion, this echographic picture can be considered a sign of partial divergence of the suture on the uterus. Signs of inflammation of the muscular layer of the uterus were also noted in the form of an increase in the vascular pattern: the appearance of sharply dilated vessels, the presence of structures with reduced echo density in the projection of the suture after cesarean section (Fig. 8-2).
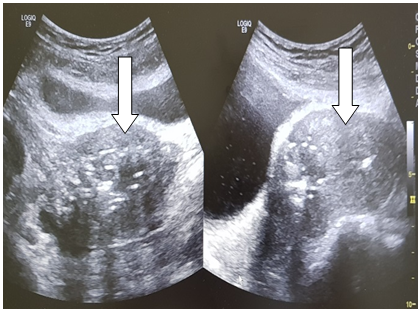 | Figure 8. Symptom of a "niche" on echography of a postoperative scar, metroendometritis |
 | Figure 9. Visualization of the uterine cavity during Doppler measurements (powerdoppler) |
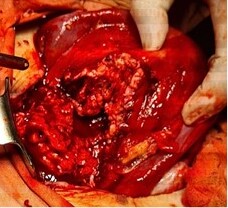 | Figure 10. Complete divergence of sutures on the uterus after СS operation on day 10. The wound is covered with fibrin, there is an inflammatory fibrin detritus of the endometrium |
 | Figure 11. After metroplasty-necroectemia, secondary sutures were applied to the uterus with secondary row vicryl knotted sutures. The integrity of the uterine scar was restored |
ACKNOWLEDGEMENTS
- I would like to express my gratitude to the staff of the Republican Perinatal Center in Tashkent for their assistance in collecting the necessary materials for scientific work, as well as for the scientific analysis of the collected materials by researchers of the Department of Pathological Anatomy of the Tashkent Medical Academy.