-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(3): 186-188
doi:10.5923/j.ajmms.20211103.05
Received: Jan. 20, 2021; Accepted: Feb. 18, 2021; Published: Mar. 15, 2021

The Prevalence and Causes of Dental Phobia in Children Aged 6-15
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJasur Rizaev1, Nargiza Ortikova2
1Doctor of Medical Sciences, Professor, Samarkand State Medical Institute, Samarkand, Uzbekistan
2PhD Student, Samarkand State Medical Institute, Samarkand, Uzbekistan
Correspondence to: Jasur Rizaev, Doctor of Medical Sciences, Professor, Samarkand State Medical Institute, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the present study was to reveal the prevalence of dental phobia in children aged 6-15 years at an outpatient dental appointment. This survey was conducted in 2020 among 100 children in Samarkand, Uzbekistan. The MDAS was used for dental anxiety measuring; the Luscher’s color test was used in children aged 6 years to assess their psycho-emotional status and own questionnaire was used to reveal the reason of the patient’s greatest fear at the dental appointment.
Keywords: Dental phobia, MDAS, Luscher’s color test, Psycho-emotional status
Cite this paper: Jasur Rizaev, Nargiza Ortikova, The Prevalence and Causes of Dental Phobia in Children Aged 6-15, American Journal of Medicine and Medical Sciences, Vol. 11 No. 3, 2021, pp. 186-188. doi: 10.5923/j.ajmms.20211103.05.
1. Introduction
- Dental anxiety and dental phobia are serious and common problems among children and can be an obstacle to the provision of high-quality dental care [1]. The term “dental fear and anxiety” is used to describe the negative feelings of children associated with the visits to the dental office [2]. A severe form of “dental fear and anxiety” is dental phobia which is characterized by the presence of excess dental fear and anxiety for at least 6 months when dental care is actively avoided [3]. Dental phobia negatively influences the oral health of children (e.g., more untreated carious lesions) [4,5,6,7]. Dental phobia is closely related to clinically significant deterioration of the oral health [8] which, in turn, leads to anxiety loopback and increased avoidance of visiting dental professionals [9]. This often means a higher likelihood of irregular dental care or even complete avoidance resulting in poor oral health [9]. The prevalence of dental fear and anxiety among persons aged 4-18 years varies from 6 to 19%, with an average prevalence of 10%. In self-reported cases the average prevalence ranged from 12 to 17% [2,10]. Five year olds children with dental anxiety showed statistically significant high rates of prevalence and intensity of caries [11]. 2-3% of patients completely avoided dental care [12].Objective: to reveal the prevalence of dental phobia in children aged 6-15 years at an outpatient dental appointment.
2. Materials and Methods
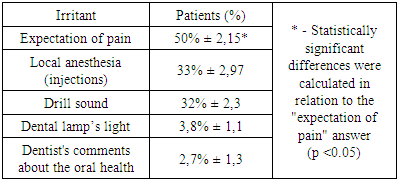
- This survey was conducted in 2020 among 100 children aged 6 to 15 years using the modified dental anxiety scale (MDAS). The MDAS includes five elements for dental anxiety measuring.Patients also noted the reason of the greatest fear at the dental appointment: 1) anesthesia, injections; 2) the sound of a drill; 3) lamp light; 4) dentist's remarks about the current oral health; 5) expectation of pain; 6) or own answer.The Luscher’s color test was used in children aged 6 years to assess their psycho-emotional status. According to Luscher’s test 4 points scored by the patient indicate a favorable emotional status, 3 points- satisfactory, 2 – unsatisfactory status (specialist’s help is required), 1 - the child is in a state of crisis and needs help of a psychologist or psychotherapist.Depending on age all children were divided into 3 groups: aged 6 (19 children), 7-11 (46 persons) and 12-15 (45). The data were statistically processed using Microsoft Excel 2010 using parametric statistics methods.The study was conducted in Samarkand state medical institute (SSMI), Uzbekistan. The study has been conducted in full accordance with the Helsinki declaration by World Medical Association. SSMI Institutional Review Board gave the approval for conducting the study and verbal informed consent from all the dentists was also obtained prior to the survey. Information from all the participating dentists was collected ensuring anonymity of the information provided.
3. Results
- It was found that 47% of children aged 7-15 years experienced dental anxiety before visiting paediatric dentist (mean MDAS score 19 ± 1.3). Further analysis of the results of the MDAS scale revealed that children aged 11-15 years were most susceptible to dental anxiety (67% of cases) (tab. 1).
|

|
4. Discussion
- Fear and anxiety are conditions that, in an evolutionary context, contribute to survival [13]. Various cognitive, neurobiological, emotional and behavioral responses are triggered when faced with a dangerous situation and these responses allow us to protect ourselves [14]. Our attention is focused on danger and the body prepares to "fight" or "flight" (adrenaline is released to increase strength and endurance, the heart beats faster to pump blood to the major muscle groups, the body begins to sweat to maintain an optimal temperature).While these “survival responses” are useful in situations where there is a real danger, in cases where there is no real threat, instinctive fear responses are not helpful and can increase distress. For example, children become anxious because they do not understand what is happening to them. Therefore, the first thing that dental practitioners can do to support anxious patients is to explain the fear response and normalize feelings of anxiety.Anxiety during dental treatment prevents the patient from fully cooperating with the dentist, leading to wasted time for the dentist, unnecessary difficulties in performing dental procedures and unsatisfactory results [15]. Based on this, dental anxiety can be considered a potential predictor of the incidence of dental caries.A study by Locker et al. [16] showed that about half of people report that their dental anxiety developed during childhood. These people tend to have more severe “dental fear and anxiety” in adulthood than people whose anxiety developed during adolescence or adulthood. Studies have also shown that children with “dental fear and anxiety” are more likely to become symptomatic rather than active users of dental services in adulthood [17].
5. Conclusions
- Thus, we can conclude that dental phobia is common among children aged 6-15 and the main risk factors for its occurrence include anticipation of pain, local anesthesia and the noise of a drill.An analysis of the scientific literature revealed that, despite the presence of studies on the study of the psycho-emotional stress of children at an outpatient dental appointment there is still no effective way to correct it, which makes it highly relevant to search for a solution to this problem.