-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(2): 160-163
doi:10.5923/j.ajmms.20211102.20
Received: Jan. 14, 2021; Accepted: Feb. 23, 2021; Published: Mar. 3, 2021

Assessment of Sensitivity of 14-3-3 (Eta) Protein and MRI of Joints in Diagnosis of Early Rheumatoid Arthritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaktuba Tashpulatova , Dildora Nabiyeva, Elnora Djurayeva, Nigora Akhmedova
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Maktuba Tashpulatova , Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of our study was to study the sensitivity of 14-3-3 (Eta) protein in the blood and conducting of MRI (magnetic resonance imaging) of the joints of the hands in the diagnosis of rheumatoid arthritis (RA) in the early stages of disease. The study included 68 patients aged 19 to 74 years (mean age 44.2 ± 3.2 years) with RA onset (meeting the EULAR / ACR criteria, 2010) with a disease duration of up to 1 year (from 6 to 52 weeks.), in the I clinic of TMA for the period 2019 - 2020. All patients underwent a general clinical and biochemical blood test, immunological blood test (rheumatoid factor (RF), anticyclic citrulline peptide (ACCP) and 14-3-3η (Eta) protein in the blood). Also, radiography (RG) of the hands was carried out, as well as MRI of the joints of the hands. Determination of 14-3-3η (Eta) protein and MRI of joints have a sensitivity comparable to that of RF, ACCP, RG and are highly effective methods for diagnosing early RA, which, in combination with other research methods, helps to establish a diagnosis of the disease at an early stage, which contributes to the timely the appointment of an adequate basic treatment.
Keywords: Early rheumatoid arthritis, Rheumatoid factor, Anticyclic citrulline peptide, 14-3-3η (Eta) protein, Magnetic resonance imaging, Radiography
Cite this paper: Maktuba Tashpulatova , Dildora Nabiyeva, Elnora Djurayeva, Nigora Akhmedova , Assessment of Sensitivity of 14-3-3 (Eta) Protein and MRI of Joints in Diagnosis of Early Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 11 No. 2, 2021, pp. 160-163. doi: 10.5923/j.ajmms.20211102.20.
Article Outline
1. Introduction
- Currently, the concept of early stage of RA is interpreted ambiguously. Various authors define it as period of time from several months to several years. Some experts identify the first 3 months of the disease as a very early stage. Scientific research, which is carried out in the framework of the problem of early arthritis, is devoted primarily to the solution of two closely related issues. Firstly, the possibilities of establishing a reliable diagnosis are being studied, and secondly, the approaches to prescribing the optimal therapy option for a given period of the disease are being worked out [1]. The problem of accurate early diagnosis of RA, which is inextricably linked with the study of the immediate and long-term outcomes of the disease, is currently especially relevant, due to the possibility of slowing down the development of the disease with the help of modern methods of treatment, provided that therapy is started early [3].
2. Purpose of the Study
- To study the sensitivity of 14-3-3 (Eta) protein in the blood of patients and to conduct MRI of RA in the early stages of disease.
3. Material and Methods
- The study included 68 patients aged 19 to 74 years (mean age was 44.2 ± 3.2 years) with RA onset (meeting the EULAR / ACR criteria, 2010) with disease duration up to 1 year (from 6 to 52 weeks), who underwent inpatient treatment in the departments of cardio-rheumatology and rheumatology and were registered at the arthrological direction of I clinic of the TMA for the period 2019 - 2020. By sex, the patients were distributed as follows: 63 women (93%) and 5 men (7%) (F: M = 12: 1). The average duration of the disease averaged 5.7 ± 0.9 months. To determine the activity of RA disease, the following indicators were used: the severity of pain in the joints, assessed by the patient on a visual analogue scale (VAS), the total activity of the disease was assessed according to the DAS28 index recommended by EULAR. To assess the functional capabilities of the RA patient, the definition of the functional class was used. The functional status of the patient was determined using the Stanford Health Assessment Questionnaire (HAQ, 1980). The laboratory examination included a general clinical and biochemical blood test, an immunological blood test: determination of the concentration of RF, ACCP and 14-3-3 (Eta) protein in the blood. To determine the degree of disease activity, ESR (mm / h) was determined according to Westergren with the release of 3 main degrees and CRP in the blood serum. Diagnostics of autoantibody panels included the quantitative determination of RF by the Waaler-Rose method, as well as ACCP and 14-3-3 (Eta) protein by the enzyme immunoassay.
4. Results and Discussion
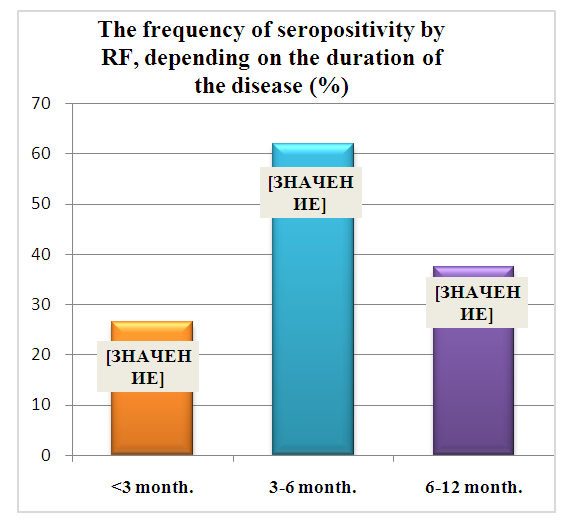
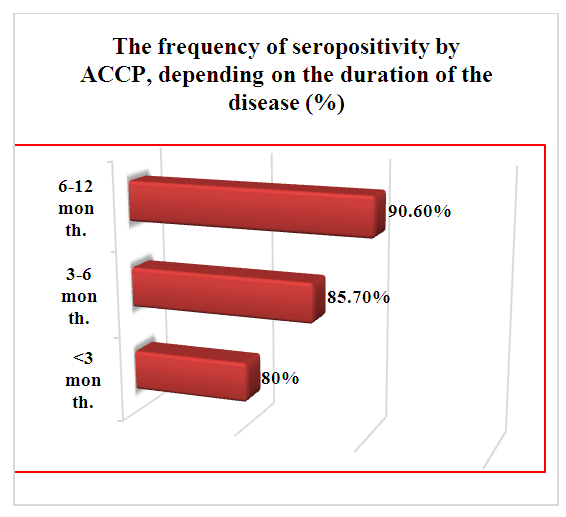
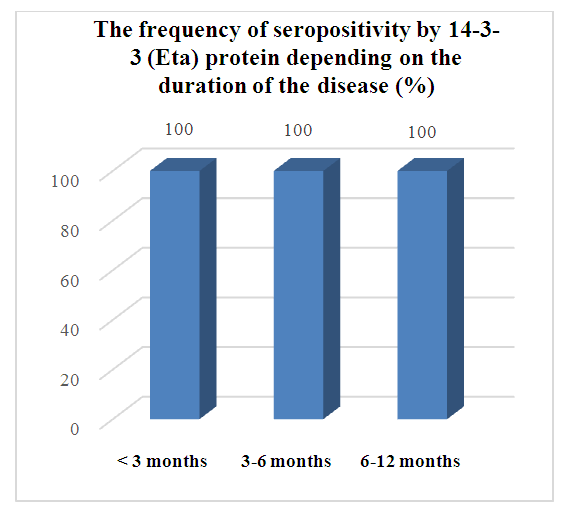
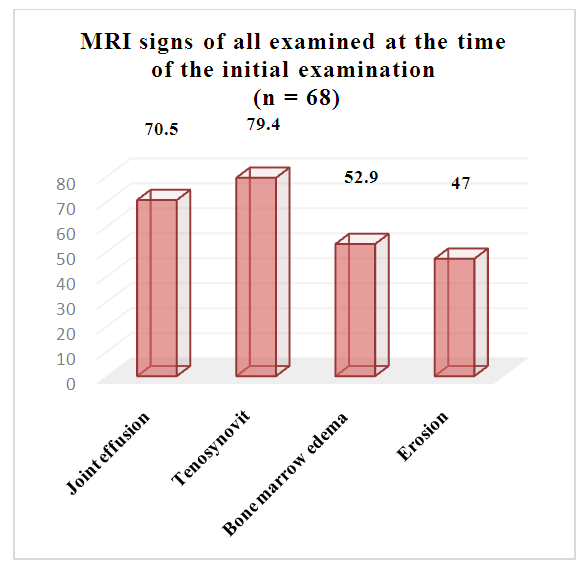
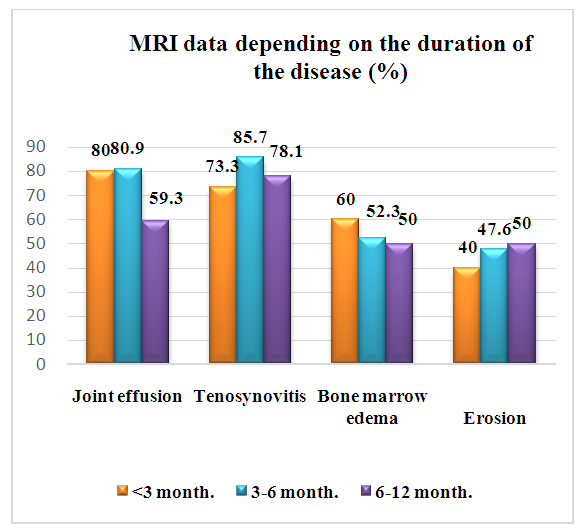
- Sero-belonging is of no small importance in the diagnosis of RA; according to the results of this study, seronegativeness was mostly noted at an early stage. According to the literature, it is known that patients who are positive for the RF have a worse prognosis for the course of the disease. However, the RF phenotype has two significant limitations. First, the specificity of this test for RA is rather low: RF is found in about 5% of healthy people, in 5-25% of elderly people, as well as in a significant number of patients with chronic diseases. Secondly, the presence of RF is not stable. The frequency of RF detection depends significantly on the duration of the disease. The results of one of the domestic studies have shown that in the first 6 months it is detected only in 15-43% of patients with RA, and subsequently some RF-negative patients become RF-positive. Under the influence of treatment, the reverse transformation is also possible [6]. With a disease duration of up to one year, 43% of patients were seropositive in the RA, and 57% were seronegative. In the group of patients with RA duration of less than 3 months, RF was detected in 27%, and with an increase in the duration of the disease, its indicator increased to 62% (Fig. 1), ACCP was determined in 80% of the examined patients with a disease duration of up to 3 months, by 12 months of illness, on average, in 90.6% of patients, this indicator was positive (Fig. 2.). 14-3-3 (Eta) protein was detected in all (100%) patients examined, regardless of the duration of the disease (Fig. 3.).
 | Figure 1 |
 | Figure 2 |
 | Figure 3 |
 | Figure 4 |
 | Figure 5 |
 | Figure 6 |
5. Conclusions
- In the early stages of the disease, 57.4% of patients were seronegative in the RF, diagnostically significant titers of ACCP were determined in 86% of patients, and at the same time, 14-3-3 (Eta) protein in the blood was determined in all (100%) patients. When analyzing radiographs of the joints in 51.5% of patients, pathological changes were not revealed, in the remaining 48.5%, certain radiological manifestations of RA were determined at the time of the initial examination. An interesting fact is that the analysis of the results of MRI of the joints in patients with early RA showed the presence of significant pathological changes in contrast than RG. The highest sensitivity and specificity for detecting erosions in RA patients was observed during MRI of the hands (47%) compared with RG (13.2%). In the absence of early erosions, bone marrow edema was determined in 52.9% of patients, which is considered a reliable precursor of erosion. Determination of 14-3-3 (Eta) protein has a sensitivity comparable to the sensitivity of ACCP and RF, and significantly exceeds them. Compared to radiography, MRI is a highly effective method for diagnosing RA, which, in combination with other research methods, helps to establish a diagnosis of the disease at early stage, which contributes to the timely appointment of an adequate basic treatment.