-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(1): 39-41
doi:10.5923/j.ajmms.20211101.10
Received: Dec. 17, 2020; Accepted: Jan. 6, 2021; Published: Jan. 15, 2021

Clinical and Laboratory Manifestations of Viral Encephalitis Depending on Immunodeficiency
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLV. Kh. Sharipova, M. M. Bakhadirkhanov, R. K. Djamaldinova, R. I. Kasimova
Republican Research Center of Emergency Medicine, Tashkent Institute of Post-Education Doctors, Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The authors investigated the effect of the patient's HIV status on the confirmed viral encephalitis clinical course and the parameters of the patients' cerebrospinal fluid. The HIV-seropositive status of patients suggests a more severe course of viral encephalitis and a longer duration of the disease together with a less optimistic prognosis for the brain functional state recovery.
Keywords: Acute viral encephalitis, Human immunodeficiency virus, Cerebrospinal fluid
Cite this paper: V. Kh. Sharipova, M. M. Bakhadirkhanov, R. K. Djamaldinova, R. I. Kasimova, Clinical and Laboratory Manifestations of Viral Encephalitis Depending on Immunodeficiency, American Journal of Medicine and Medical Sciences, Vol. 11 No. 1, 2021, pp. 39-41. doi: 10.5923/j.ajmms.20211101.10.
1. Introduction
- Viral encephalitis (VE) makes up 80–89% of all etiological agents causing encephalitis [4]. VEs are a heterogeneous group of pathologies that include primary viral encephalitis, for example, herpetic encephalitis and secondary post-infectious acute disseminated encephalitis (encephalo-myelitis). Viral encephalitis requires mandatory emergency medical intervention and, of course, early correct diagnosis [3].The nervous system is in second place after the immune system by the frequency of lesions to organs and systems at HIV infection. In this regard severe dysfunctions of the nervous system are develo0ped in significant proportion of patients. Previously, at the onset of neuroAIDS clinical manifestations the course of HIV infection has steadily progressed up to the lethal outcome. Today, the commonly used antiretroviral therapy (ART) has significantly improved the prognosis of AIDS. It drew attention to the lesions of the nervous system in HIV infection as a factor determining the life expectancy of patients and the development of new directions for the treatment of neuro AIDS. In high-income countries, the introduction of ART has dramatically reduced the incidence of opportunistic infections (OIs) of the central nervous system (CNS) from 13-1 cases per 1000 patients per year in 1996-1997 to 1-0 per 1000 in 2006-2007. OIs most often affecting the central nervous system are: cerebral toxoplasmosis, progressive multifocal leukoencephalopathy (PML), cytomegalovirus (CMV), central nervous system tuberculosis, cryptococcal meningitis, primary central nervous system lymphoma. OI of the central nervous system should be suspected in all patients with HIV at clinical stage 4, and it may be the first clinical manifestation of HIV. Many CNS OIs are characterized by nonspecific symptoms such as fever and lethargy. A combination of symptoms: the addition of a headache or the duration of headaches for more than 3 days, the onset of seizures or changes in the mental state, indicate an acute focal brain lesion [Garvey L, 2011].The immediate and long-term outcomes of acute VE in the modern world are often unfavorable. There is a high degree of disability together with the high mortality in patients with acute EV; therefore, it is necessary to expand knowledge about this pathology [7].The urgency of the VE problem is due to the high severity of this disease, a high mortality rate (10-20%) and a high incidence of neurological complications with an extremely unfavorable prognosis [6].The main diagnostic criteria of CNS infections are clinical presentation of cerebrospinal fluid (CSF) changes and radiographic methods.The optimal diagnostic test is a combination of PCR and antibody detection in the patients' cerebrospinal fluid (CSF) [5,8]. Despite the use of modern diagnostic laboratory research methods, it was not possible to determine the etiology of encephalitis in some patients. The etiology of 30–62% of encephalitis remains undeciphered in world practice [2,1].Aim of the study was the estimation of the patient's HIV status effect on the confirmed viral encephalitis clinical course and the parameters of the patients' cerebrospinal fluid.
2. Material and Methods
- Our study involved 124 patients with viral encephalitis. We conducted a rapid HIV test for all patients. 52 patients who underwent an ELISA study to detect antibodies to the HIV virus were diagnosed as “HIV-seropositive”. Some of the patients (46) knew about their “HIV-seropositive” status (by relatives’ words). 26 patients had this status for the first time. Patients were divided into 2 groups based on HIV status: Group I - patients with HIV-seronegative status and Group II - patients with HIV-seropositive status. In group I 25 (34.7%) patients were diagnosed with enterovirus, herpes simplex virus (HSV-1/2) – in 12 (16.7%) patients, Epstein-Barr virus – in 6 (8.3%), cytomegalovirus (CMV) – in 2 (2.8%) cases. CMV dominated in group II – in 13 (25%) patients, Epstein-Barr virus – in 8 (15.4%) cases, HSV-1/2 – in 2 (3.8%) patients.The clinical manifestations of VE were characterized by an acute onset with a temperature reaction in all patients from sub febrile digits to severe fever. All patients had symptoms of intoxication: diffuse headache was characterized as “pressing” in 94 (75.8%) and “bursting” in 30 (24.2%) of our patients; nausea and vomiting that did not bring relief were recorded in 78 (62.9%) patients.112 (90.3%) patients had movement disorders: 46 (37.1%) had paresis of one arm, 66 (53.2%) had hemiparesis. Sensory disorders were diagnosed in 94 (75.8%) patients. Moderate transient bulbar disorders were detected in 79 (63.7%) cases, changes in the oculomotor nerves were recorded in 37 (29.8%) patients. Facial nerve paresis of the central type was revealed in 23 (18.5%) cases. Signs and symptoms of cytomegalovirus -encephalitis were nonspecific: drowsiness, fever, disorientation, confusion, and apathy. Studies of brain neuroimaging in cytomegalovirus -encephalitis have shown an increase in signal intensity on the ependymal surfaces of the ventricles, which is typical for periventricular inflammation). Epstein-Barr virus -encephalitis and herpes simplex virus -encephalitis were characterized by a relatively abrupt onset of changes in mental status and / or focal neurological signs. Neurological status was estimated with the use of the following scales:The Glasgow Coma Scale allowed evaluating any patient regardless of the consciousness level or other disorders. Estimation of the consciousness state was carried out on the basis of summing up the points obtained when checking clinical signs, while taking into account the best of the identified reactions [9]. Interpretation of the results obtained was carried out on a point system: 15 points - clear consciousness, 13-14 points - stunning, 9-12 points - stupor, 4-8 points - coma, 3–0 points - deep coma.Ashworth Scale is used to measure spasticity and evaluation of its treatment effectiveness; it measures the severity and frequency of resistance to passive movements. The result is estimated by the doctor on a five-point scale ranging from 0 to 4. The test consists in the doctor's movement of the patient's limbs in the full range of motion and a subjective assessment of muscle tone during flexion in the following order: elbow, wrist, fingers. Points are distributed as follows:0. – The tone is not increased.1. – Slight increase in muscle tone (initial tension and rapid subsequent relief).2. – Moderate increase in tone throughout the range of motion, but the arm flexes / extends easily.3. – Significant increase in muscle tone (passive movements are difficult).4. – Inability to fully bend or unbend the paretic part of the limb.Barthel Index for Activities of Daily Living (ADL):In the Barthel scale the scores from 0 to 45 correspond to severe disability (significant or complete impairment of neurological functions); 50 - 70 points - moderate disability (limitation of neurological functions); 75 - 100 points - minimal limitation or preservation of neurological functions. The Ashworth Scale subjectively measured the severity and frequency of resistance to passive movements; this scale also stated spasticity in all patients.
3. Results and Discussion
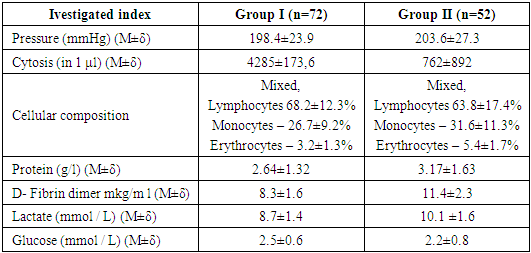
- The Barthel Index stated the dependence of our patients on any kind of help, physical or verbal; they needed constant supervision, which made them addicted (Tab. 1).
|

|
4. Conclusions
- The HIV-seropositive status of patients suggests more severe course of viral encephalitis and a longer duration of the disease together with a less optimistic prognosis for the brain functional state recovery.