-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(1): 36-38
doi:10.5923/j.ajmms.20211101.09
Received: Dec. 14, 2020; Accepted: Jan. 5, 2021; Published: Jan. 15, 2021

Tablet Shaped Battery Ingestion in 3 Years Old Child (Case Report)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkilov Kh. A., Asadullaev D. R.
Republican Research Centre of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Foreign bodies of the gastrointestinal tract are one of the most pressing problems in pediatric surgery and gastroenterology. This review discusses the prevalence of gastrointestinal tract foreign bodies in children, and describes in detail the problems of current diagnostic and treatment methods.Authors have analyzed a case of successful treatment of tablet shaped battery ingestion in 3 years old baby. Short reviews of literature, clinical and instrumental data and surgical treatment result have been presented.
Keywords: Foreign body, Esophagus, Tablet battery, Chemical burn
Cite this paper: Akilov Kh. A., Asadullaev D. R., Tablet Shaped Battery Ingestion in 3 Years Old Child (Case Report), American Journal of Medicine and Medical Sciences, Vol. 11 No. 1, 2021, pp. 36-38. doi: 10.5923/j.ajmms.20211101.09.
Article Outline
1. Introduction
- Gastrointestinal foreign bodies are common problems in children. Some of the swallowed foreign bodies are particularly harmful and life-threatening: they include batteries, magnets and various sharp objects [1-6]. The frequency of tablet shaped batteries being swallowed by children has significantly increased for recent years. Batteries made up to 15% of the total number of gastrointestinal (GI) tract foreign bodies (FB) in children. At average 300 patients with FB of GI tract are admitted to the pediatric surgery department annually. The frequency of batteries swallowing is approximately 40–45 cases annually which often lead to serious consequences. The peak incidence occurs at the age of 6 months to 5 years [7-8,3,9-11]. The widespread use of toys, household electronic devices and battery-operated mechanisms, the attractive shape of the batteries contribute to an increase of the frequency of their ingestion, especially by young children. According to the National Poison Data System, there were 56,535 esophageal injuries by batteries in children in the United States from 1985 to 2009. In 65% of cases batteries were swallowed by children under 6 years. The peak of these incidents occurred at the age of 1-3 years. Lethal outcomes were rare, however, in most cases, severe consequences occurred in children under 4 years old who could not speak at all. The causes of death are different - a lack of anamnesis and non-specificity of symptoms (vomiting, cough, fever, loss of appetite, etc.), the presence of esophageal fistulas. Moderate and severe injuries were often associated with particularly large alkaline and lithium batteries (20 mm or larger) in children under 4 years. Thus, the main damaging factors of esophageal FB in children under 4 years old were its chemical composition and physical pressure on the esophageal wall. As an example, we present our own observation of prolonged standing (more than 4 months) of a tablet shaped battery in the esophagus of a younger age group child and the results of its successful treatment.
2. Case History
- A child of 2 years 8 months was admitted to the Department of Pediatric Surgery of the Republican Research Centre of Emergency Medicine. Complaints at admission were difficulty in swallowing thick food, fever, lethargy, decreased appetite and frequent colds. From the anamnesis it became known that during the last four months, while eating, the child vomited up to 2-3 times a week. The child was consulted by a pediatrician, ENT doctor and neurologist. No pathology was revealed. Then the child was referred to a pediatric surgeon and a plain chest X-ray was performed. Chest X-ray revealed FB of the upper parts of the GI tract. An attempt of the FB endoscopic removal was made, but unsuccessfully. Then the patient was referred to our Centre.At admission the child was passive. Cardiopulmonary activity was satisfactory. There was no subcutaneous emphysema in the neck and chest area. The abdomen was soft, regular, not swollen and accessible on palpation, painless. There were no symptoms of peritoneal irritation. Physiological functions were normal. At contrast esophagography (trazograph 76%), estvasation was not observed. The FB of the cervical esophagus was determined (Fig. 1).
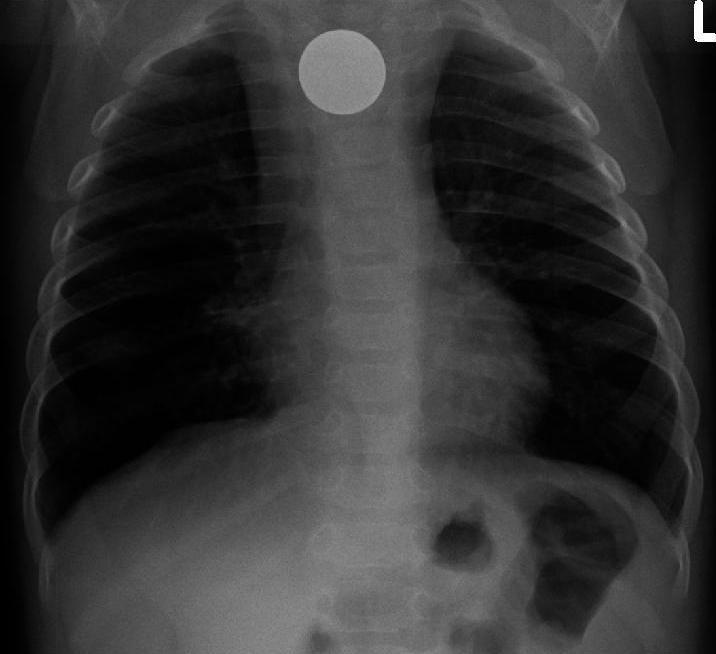 | Figure 1. Plain radiography in direct projection: at the Th 2-Th4 level, a round-shaped radiopaque FB with a diameter of 2 cm is determined |
3. Performed Procedures
- A repeated endoscopic examination of the esophagus was performed and it revealed the following: at a distance of 1.5 cm from the orifice of the esophagus, a round foreign body was visualized - a battery, the area was covered with fibrin, deformation and narrowing of the esophageal lumen to 9 mm due to edema were also noted. A second attempt of removing foreign body was unsuccessful. The child was performed surgery due to unsuccessful attempts of removing esophageal FB: upper midline laparotomy, gastrostomy according to the Stamm - Sen - Kader, left-sided colitomy, esophagotomy, removal of a foreign body from the lumen of the cervical esophagus, suturing of the anterior-left wall of the cervical esophagus, sanitation, drainage of paraesophageal tissue. Postoperative diagnosis: foreign body of the cervical esophagus (battery), complicated by a pressure ulcer in the anterior left wall of the cervical esophagus and infiltration of the paraesophageal membrane in the neck.
4. Obtained Results
- The postoperative period was uneventful, therapy included the use of a wide range of antibacterial therapy, regenerative drugs, against the background of which the inflammatory phenomena were arrested. A narrowing of the esophagus up to 15 mm was noted on the control contrast esophagography performed on the 15th day after the operation (Fig. 2).
 | Figure 2. Contrast esophagography after surgery: there is a narrowing of the esophagus lumen and no contrast extravasation |
5. Conclusions
- Esophageal foreign bodies are a serious problem in pediatric surgery. This observation demonstrates the nonspecificity of the clinical picture, difficulties in collecting anamnesis, clarifying the fact that children swallowed foreign bodies. The doctor of any specialty, most often the pediatrician, who is the first to contact the patient, should always be on the alert. For timely diagnostics, at the slightest suspicion of a foreign body of GI tract, overview radiography should be performed. And if foreign body is detected, the child should be sent to a specialized surgical hospital that has the ability for endoscopic treatment to avoid the development of serious urgent complications.