-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(1): 33-35
doi:10.5923/j.ajmms.20211101.08
Received: Dec. 13, 2020; Accepted: Dec. 30, 2020; Published: Jan. 15, 2021

The Role of Benign Polyps in the Formation of a Precancerous State of the Gallbladder
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEgamberdiyev Kuvonchbek1, Nizom Ermatov2, Khaitov Akbar1
1Assistants, Department of General Surgery and Orthopedics Traumatology of the Urgench Branch of Tashkent Medical Academy, Khorezm, Uzbekistan
2Head of the Department of Hygiene of Children and Adolescents and Food Hygiene of the Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

According to autopsy studies, gallbladder cancer is the most common malignant neoplasm of the biliary tract, accounting for 80–95% of all biliary cancer cases worldwide. Purpose of the study. Determine the role of benign polyps in the formation of a precancerous state of the gallbladder. Materials and research methods. To achieve this goal, the results of treatment of 45 patients with precancerous diseases of the gallbladder were analyzed. Depending on the cause of the etiological factor that caused the precancerous state of the gallbladder, all patients were divided into 2 groups: group 1 - patients who found stones in the gallbladder on ultrasound examination (n = 26), moreover, patients who had stones up to 3 cm was 17 people, and patients who, according to ultrasound, found stones more than 3 cm (n = 9), group 2 - patients who, according to microbiological studies, had a history of infectious processes (n = 19), and patients who, according to microbiological researches were identified as the causative agent of Hellicobacter billis - 11 patients, and 8 patients had chronic typhoid infection as an etiological factor. Research results. Among all examined (n = 45), divided by gender, 23 patients were men, 22 were women. Gallstones were more common in men than in women (14 vs 12). Biliary polyps were found in all examined patients (100%). The average age at the time of the examination was 49.3 ± 12.0 years. Among the examined patients, 2 (4.45%) had gallbladder hamartoma as an etiological factor, and 1 (2.23%) had mixed infection. 4 (8.89%) patients had a gallbladder adenoma, i.e. her hyperplasia. In the quality of heterotopia, pathology of the liver and gallbladder was found in 3 (6.67%). The following drugs can be used as adjuvant therapy after surgical treatment: gemcitabines, fluoropyrimidines. Monotherapy has a limited effect. The combination of chemotherapy with gemcitabines and cisplastins gives better survival than simple gemcitabine administration (p≤0.05, U-0.03467, r = 0.116528, χ2 = 0.87514). Conclusions: According to the conducted studies, as an etiological factor, the increased content of the triglyceride fraction was higher in patients with a body mass index of 24.32 ± 3.54 with a confidence interval of 95% (p≤0.05, U-0.07833), which indicates violation of fat metabolism and lipolysis in the liver, as a result of which the synthesis of apoliprotein E is disrupted, which leads to the accumulation of high-density lipoproteins and the possible formation of gallbladder polyps, as a possible harbinger of precancerous conditions of the gallbladder.
Keywords: Precancerous diseases of the gallbladder, Benign polyps, Fraction of triglycerides, Ultrasound procedure, Microbiological examination
Cite this paper: Egamberdiyev Kuvonchbek, Nizom Ermatov, Khaitov Akbar, The Role of Benign Polyps in the Formation of a Precancerous State of the Gallbladder, American Journal of Medicine and Medical Sciences, Vol. 11 No. 1, 2021, pp. 33-35. doi: 10.5923/j.ajmms.20211101.08.
Article Outline
1. Introduction
- According to autopsy studies, gallbladder cancer is the most common malignant neoplasm of the biliary tract, accounting for 80–95% of all biliary cancer cases worldwide [6]. It ranks sixth among gastrointestinal cancers. However, global rates of gallbladder cancer show striking variability, reaching epidemic levels for some regions and ethnic groups. The basis for this variation is likely to lie in differences in environmental exposure and intrinsic genetic predisposition to carcinogenesis [15]. These risk factors differ geographically and among ethnic groups. In most cases, gallbladder cancer develops within 5–15 years, when metaplasia develops into dysplasia, carcinoma in situ, and then into invasive cancer [19]. Progression often happens quickly and imperceptibly, which portends a bleak prognosis. A satisfactory outcome depends on early diagnosis and surgical resection [2]. Despite this potential for cure, less than 10% of patients have tumors that need to be resected during surgery, while almost 50% have lymph node metastases [8]. Even after surgery, most patients progress to metastases, highlighting the importance of improving adjuvant therapy. Lesions that protrude from the wall of the gallbladder into the interior of the gallbladder are called gallbladder polyps (GP) [11]. In most patients, the diagnosis is made incidentally by routine abdominal ultrasound or after cholecystectomy for gallstones or biliary colic. Although most gallbladder polyps are benign in nature, malignant polyps are present in some cases, and early detection and proper early assessment are important for treatment and long-term survival [1,3,4,5,7,9,10,12,13,14]. The main goal of treatment for gallbladder polyps is to prevent the development of gallbladder carcinoma.The term "polypoid lesions of the gallbladder" refers to a wide range of findings. Gallbladder polyps are classified as either benign or malignant. Benign prostatic veins are subdivided into pseudotumors (cholesterol polyps, inflammatory polyps; cholesterolosis and hyperplasia), epithelial tumors (adenomas), and mesenchymal tumors (fibroma, lipoma, and hemangioma). Malignant prostatic gallstones are carcinomas of the gallbladder. A poor prognosis for patients with gallbladder carcinoma means that it is important to distinguish between benign polyps and malignant or precancerous polyps [16].The prevalence of gallbladder polyps was 4.3–6.9%. Polypoid lesions of the gallbladder include many pathological types. [20] Although there are some differences reported, the prevalence of polypoid lesions of the gallbladder is reported in 2–12% of cholecystectomy specimens, which probably depends on the indication for cholecystectomy [17,18].
2. Purpose of the Research
- Determine the role of benign polyps in the formation of a precancerous state of the gallbladder.
3. Materials and Methods
- To achieve this goal, the results of treatment of 45 patients with precancerous diseases of the gallbladder were analyzed. Depending on the cause of the etiological factor that caused the precancerous state of the gallbladder, all patients were divided into 2 groups: group 1 - patients who found stones in the gallbladder on ultrasound examination (n = 26), moreover, patients who had stones up to 3 cm was 17 people, and patients who, according to ultrasound, found stones more than 3 cm (n = 9), group 2 - patients who, according to microbiological studies, had a history of infectious processes (n = 19), and patients who, according to microbiological researches were identified as the causative agent of Hellicobacter billis - 11 patients, and 8 patients had chronic typhoid infection as an etiological factor.All patients signed a voluntary written consent to participate in the experiment. Statistical processing of the results was carried out using the Student-Fischer, Kraskes-Wallis test, the nonparametric Mann-Winney test, and the Wilconson test for indirect samples.
4. Results
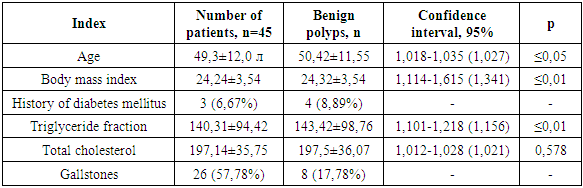
- Among all examined (n = 45), divided by gender, 23 patients were men, 22 were women. Gallstones were more common in men than in women (14 vs 12). Biliary polyps were found in all examined patients (100%). The average age at the time of the survey was 49.3 ± 12.0 years.
|
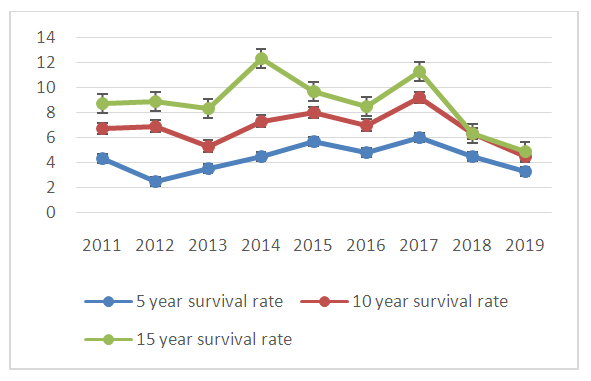 | Figure 1. Survival of patients with precancerous conditions of the gallbladder |
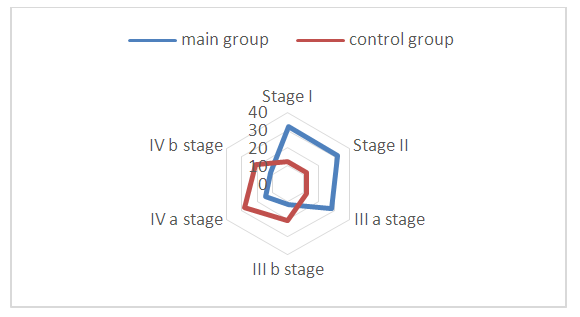 | Figure 2. Distribution of patients depending on the stage of the tumor |
5. Conclusions
- According to the conducted studies, as an etiological factor, the increased content of the triglyceride fraction was higher in patients with a body mass index of 24.32 ± 3.54 with a confidence interval of 95% (p≤0.05, U-0.07833) which indicates metabolic disorders fat and lipolysis in the liver, as a result of which the synthesis of apoliprotein E is disrupted, which leads to the accumulation of high density lipoproteins and the possible formation of gallbladder polyps, as a possible harbinger of precancerous conditions of the gallbladder.