-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2021; 11(1): 25-32
doi:10.5923/j.ajmms.20211101.07
Received: Dec. 3, 2020; Accepted: Dec. 31, 2020; Published: Jan. 15, 2021

USS Diagnostic Score in High-Altitude Trauma
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. M. Khadjibaev, J. A. Djuraev, P. K. Sultanov, Khadjayarov N. P.
Republican Research Centre of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction The frequency of abdominal organs and retroperitoneal space injuries at combined catatrauma remains high. Aim of research is to study the diagnostics methods at combined abdominal organs and retroperitoneal space injuries. Material and methods We analyzed diagnostics and treatment results of 180 victims of high-altitude trauma with combined injuries of the abdomen admitted to the surgical department of the Republican Research Centre of Emergency Medicine. Radiological and CT examinations, endosurgical interventions were performed to all patients. Results Combined injuries among patients with abdominal injuries were detected by instrumental methods in 94.9% and 88.3% of cases. The most frequently combined abdominal injuries were noted in patients with injuries of the chest organs (17.7% and 6.3%); head and extremities (10.1% and 2.7%); head + chest + pelvis + extremities (7.6% and 11.7%), head + chest + extremities (8.9% and 10.8%). Isolated abdominal injury was found in 5.1% and 11.7% of cases in the main and control groups. Injuries of abdominal organs at isolated or combined abdominal trauma during catatrauma were mainly manifested by ruptures of parenchymal organs with hemoperitoneum. Mortality among catatrauma victims with isolated and combined abdominal injuries was 17.7% in the main group and 27% in the control group. Conclusion It is very important to recognize simultaneously all the injuries immediately after the victim admits the hospital, while assessing the dominant ones. This need is imperative, vital, justified, urgent, as it is the motive for determining surgical tactics.
Keywords: Polytrauma, Combined injury, Catatrauma, Solated injury, Diagnostics, Abdominal injury
Cite this paper: A. M. Khadjibaev, J. A. Djuraev, P. K. Sultanov, Khadjayarov N. P., USS Diagnostic Score in High-Altitude Trauma, American Journal of Medicine and Medical Sciences, Vol. 11 No. 1, 2021, pp. 25-32. doi: 10.5923/j.ajmms.20211101.07.
1. Introduction
- Polytrauma has been one of the most frequent problems of emergency surgery for recent years [1]. In peacetime, polytrauma most often occurs as a result of traffic accidents and when falling from a height [1-3]. They are characterized by severe combined injuries of various organs and systems [1-2]. Severe injuries of the brain and spinal cord internal organs of the chest and abdominal cavity dominate and become the direct cause of a victim’s death [4,2,5]. The combination of abdominal organs trauma with injuries of other anatomical areas of the body aggravates the condition of the victim, significantly complicates the diagnostics and worsens the prognosis [4,2,5]. Diagnostics of the abdomen injuries with combined catatrauma is significantly difficult due to the presence of a coma in most victims as a result of a traumatic brain injury (TBI) [6-9]. The presence of the brain compression, massive internal bleeding, multiple fractures of the ribs and pelvic bones, the development of fat embolism severely limit, and sometimes exclude the use of special investigation methods (radiological, contrast, instrumental, etc.) [10-11,3,12]. The clinical picture characterized by a large polymorphism, as a rule, does not correspond to the nature and severity of injury [5,13]. In addition, there are various factors of catatrauma to be the cause of it: the heterogeneous nature of the traumatic forces and places of their application, sometimes significantly remote from the projection of the injured organ; the different nature and degree of injury at the same traumatic force [14-16]. Mortality of catatrauma victims with combined injuries of the abdominal cavity and retroperitoneal space remains high and amounts 40-60% [14,17-18].The aim of our study was to improve the diagnostics of abdominal organs and retroperitoneal space injuries at combined catatrauma.
2. Materials and Methods
- We analyzed the diagnostics and treatment results of 190 victims of high-altitude trauma with combined injuries of the abdomen from 2010-2015, who were hospitalized to the Republican Research Center of Emergency Medicine. There were 158 (83.2%) males and 32 (16.8%) females. The age of patients varied from 15 to 80 years (mean age made up 35.83 years).The patients were divided into two groups: main group (79) and control group (111). The difference between the main and control groups of patients was in the ultrasonic gradation of free fluid volume in the abdominal cavity and, accordingly, in the tactics of surgical treatment. Ultrasound was performed in dynamics after 1, 3 hours, 6 and 12 hours from the time of admission to clarify the ongoing bleeding.
3. Results
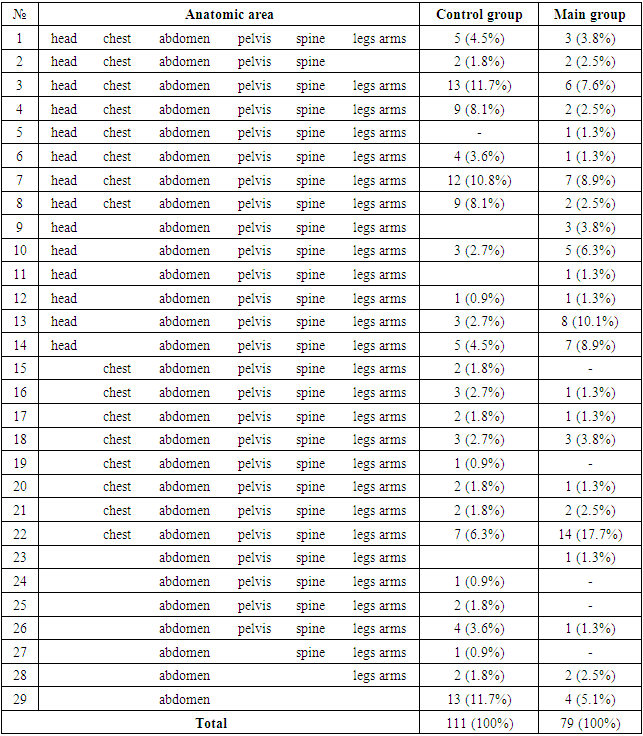
- Сombined injuries were detected among patients with abdominal injuries in 94.9% and 88.3% of cases. Moreover, a combination of 6 areas was identified in 3.8% and 4.5% of cases; 5 areas - in 11.4% and 15.3% of cases; 4 areas - in 24.1% and 31.5% of the victims; 3 areas - in 25.3% and 20.7% and 2 areas - in 30.4% and 16.2% of cases, respectively, for the main and control groups (Tab. 1). The most frequently combined abdominal injuries were noted in patients with injuries of the chest organs (17.7% and 6.3%); head and extremities (10.1% and 2.7%); head + chest + pelvis + extremities (7.6% and 11.7%), head + chest + extremities (8.9% and 10.8%). Isolated abdominal injury was found in 5.1% and 11.7% of cases in the main and control groups.
|
|

|
 | Figure 1. Ultrasound of the abdominal cavity of patient K. with catatrauma. Free fluid around the liver |
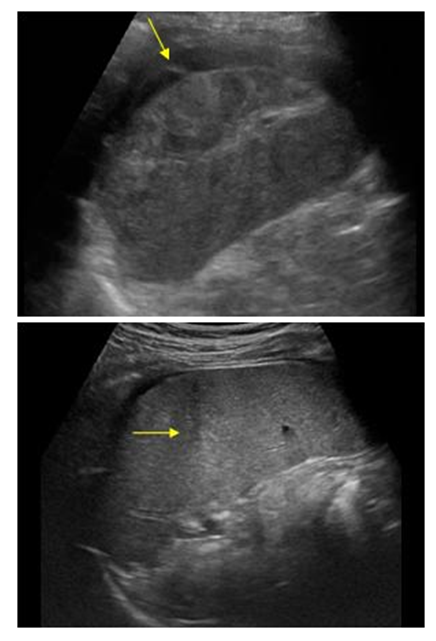 | Figure 2. Ultrasound of the abdominal cavity of patient B. with catatrauma. Free fluid around the spleen |
|
|
4. Discussions
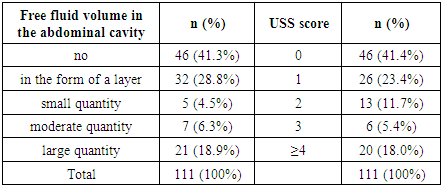
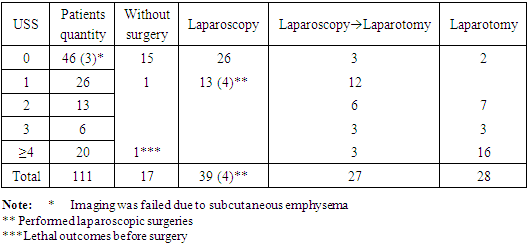
- Ultrasound diagnostics is the most common non-invasive method for diagnosing injury of internal organs during polytrauma [20,12]. Its advantage is portability, accuracy and quick investigation. The main task of ultrasound in our research was to detect free fluid (blood) in the cavities. The nature of the parenchymal organ injury was judged by the change of the size and configuration of the organ and the presence of increased echogenicity zones [21]. The method deserves serious attention for the diagnostics of internal organs injuries in patients with combined abdominal catatrauma. It is simple and accessible to use. It can be used both in the emergency room, in the intensive care room, and in the operating room, including intraoperative diagnostics. In the 90s, they offered a ball score for determining the amount of fluid in the abdominal cavity by its thickness (Ultrasound Score). So, in 1994, Huang M. introduced physiological saline during diagnostic peritoneal lavage and he measured the separation of the peritoneum leaves by ultrasound examination. The result of his research was the proposal to equate every 2 mm of free fluid in the abdominal cavity with one point and to carry out surgical treatment at a score of ≥3. Mc Kenney K.L. in 1996, examining 4 sections of the abdomen (subphrenic, subhepatic, periolane and pelvis) proposed a counting system based on the estimation of the antero-posterior maximum fluid size detected in the abdominal cavity. Mc Kenney K.L. offered surgery in the presence of free fluid ≥2cm in the abdominal cavity. In 2001, Sirlin C.B. suggested ranking by one point in the presence of free fluid in each of the 7 areas of the abdominal cavity [22]. Moreover, every 10 mm of free fluid in one area of the abdominal cavity amounts one point. For example, up to 10 mm of free fluid in the subhepatic region is equal to one point, up to 20 mm - two points, etc. If there is free fluid up to 10 mm in the subhepatic region, in the right lateral canal and in the small pelvis, then it will be evaluated at 3 points. The higher the score, the higher is the likelihood of the abdominal organs injury and the need for surgical intervention.According to our studies results, abdominal organs requiring emergency surgery were revealed in 10.9% of cases in patients with a “0” USS hemoperitoneum score. In 2 patients during the examination free gas was revealed in the abdominal cavity due to rupture of the walls of the stomach and small intestine, which required an urgent laparotomy. In 3 patients laparoscopy revealed injury of the spleen (in one case) and liver (in two cases): in the first case 400 ml of fresh blood with clots were detected intraoperatively, in the second and third ones - 100 ml and 200 ml, respectively. It is, probably, connected with poor ultrasound imaging of the abdominal organs due to the evident subcutaneous emphysema of the anterior abdominal wall as the result of combined injury of the chest organs. It should be said that at high-altitude trauma, the mechanogenesis of organ injury has its own characteristics, in particular, the heterogeneous nature of the traumatic forces and their application [14,16]. Obviously, it determined the two-moment rupture of the parenchymal organs and the absence of a sufficient quantity of free fluid in the abdominal cavity at the time of injured persons’ admission to the hospital. In our opinion, in this case, it is necessary to observe a patient with mandatory dynamic ultrasound monitoring of the abdominal cavity.Patients with a score "1" in 61.5% of cases had injuries of the abdominal parenchymal organs of various degrees. In 4 cases injuries in the form of tears of the liver and spleen capsules (I degree according to AIS) [23] became possible to be eliminated by laparoscopic means. And in 12 cases, conversion laparotomy was performed as a result of ruptures of the liver and / or spleen requiring closure of the liver rupture or splenectomy. In such situations, laparoscopy is necessary for the timely detection of internal organs injuries.Victims with a USS score of equal to or more than “2” in 100% of cases needed emergency laparotomy, as laparoscopy revealed 8 cases of splenic rupture of the II and III degree requiring laparotomy. In one of them, spleen damage was combined with rupture of the kidney, in one - with rupture of the bladder, in 2 cases - with ruptures of the liver. Victims with a USS score of equal to or more than “2” in 100% of cases needed emergency laparotomy, as laparoscopy revealed 8 cases of splenic rupture of the II and III degree requiring laparotomy. In one of them, spleen injury was combined with the kidney rupture, in one - with rupture of the bladder, in 2 cases - with ruptures of the liver. To evaluate the quantity of free fluid in the abdominal cavity in the main group we have already used USS ultrasonic gradation (Fig. 3).
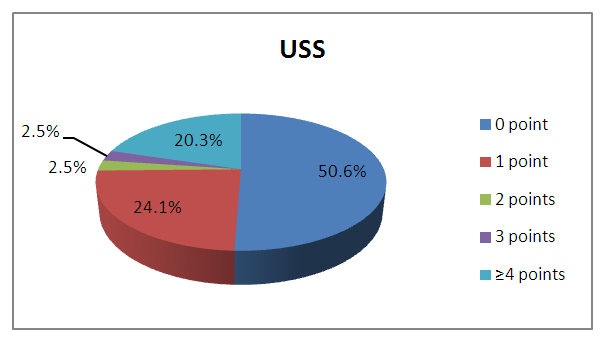 | Figure 3. The volume of free fluid in the abdominal cavity according to USS data in the main group |
|
5. Conclusions
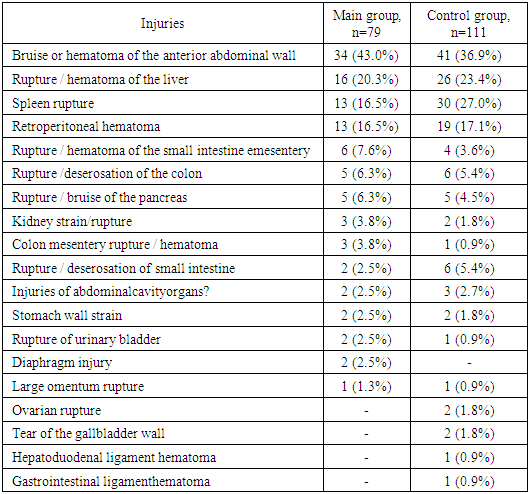
- Thus, injuries of the abdominal organs at an isolated or combined abdominal trauma during catatrauma had a multiple nature and they were mainly manifested by ruptures of parenchymal organs with hemoperitoneum. Mortality among catatrauma patients with isolated and combined abdominal injuries was 17.7% in the main group and 27% in the control group. Our experience allows us to consider that the structure of the diagnostic search for combined abdominal catatrauma can be represented as follows: primary determination of the patient’s severity according to the clinical examination and the ascertainment of the need for resuscitation aid, the identification of life-threatening complications that need to be eliminated immediately (cardiac and respiratory arrest, asphyxiation, external and internal bleeding), the identification of the dominant damage and its role in the severity of the patient’s condition according to clinical and para-clinical examination methods data (traumatogenesis); diagnostics of injuries aggravating (non-aggravating) the course of the leading trauma.The below mentioned principles should be subject to a diagnostic process that is strictly regulated and corresponding, in our opinion, to the following requirements:1) Simultaneous recognition of all available injuries immediately after the patient arrives to the hospital, while assessing the dominant ones. This need is imperative, vital, justified, urgent, as it is the motive for determining surgical tactics.2) Carrying out diagnostic measures in the anti-shock zone of the admission department against the background of intensive care and resuscitation aids aimed at eliminating life-threatening injuries, which requires determining the priority of diagnostic measures.3) To assess the ultrasonic gradation of free fluid in the abdominal cavity, it is necessary to use a USS score based on which the treatment tactics of the abdominal organs injuries is determined.