-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(12): 1024-1027
doi:10.5923/j.ajmms.20201012.20
Received: Nov. 12, 2020; Accepted: Dec. 11, 2020; Published: Dec. 26, 2020

Morphology and Morphometry of Ileum of the Newborn
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhaitov Akbar1, Nizom Ermatov2
1Assistant, Department of General Surgery and Orthopedics Traumatology of the Urgench Branch of Tashkent Medical Academy, Khorezm, Uzbekistan
2Head of the Department of Hygiene of Children and Adolescents and Food Hygiene of the Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Khaitov Akbar, Assistant, Department of General Surgery and Orthopedics Traumatology of the Urgench Branch of Tashkent Medical Academy, Khorezm, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

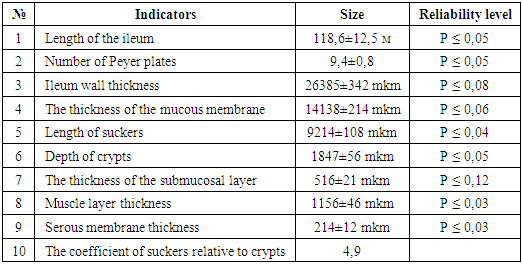
The main functions of the ileum testify to the perfection of its morphofunctional indicators. This study aimed to study the anatomical, histotopographic, and morphometric features of the lateral intestinal wall of newborn who died of traumatic brain injury at birth. The length of the ileum was 118.6 ± 12.5 ml in boys, shorter in girls - 104.3 ± 8.5 ml, the average number of peyer's patches was 9.4 ± 0.8. It was found that the epithelium covering the mucous membrane is single-layered, in some places multi-layered, their nuclei are disordered, the special plate is rich in histiogenic and lymphoid cells, which are differentiated to varying degrees. It was observed that the number of peyer's patches in the submucosal layer is relatively small, the lymphoid follicles in them completely occupy the submucosal layer and the special plate, the reticular and lymphocyte cells in them are sparse. While the wall thickness averaged 26,385 ± 342 μm, almost half of it corresponded to the mucous membrane, the suckers and crypts in it, and the rest to the submucosal, muscular, and serous membranes.
Keywords: Newborn, Small intestine, Ileum, Anatomy, Histotopography, Morphometry
Cite this paper: Khaitov Akbar, Nizom Ermatov, Morphology and Morphometry of Ileum of the Newborn, American Journal of Medicine and Medical Sciences, Vol. 10 No. 12, 2020, pp. 1024-1027. doi: 10.5923/j.ajmms.20201012.20.
Article Outline
1. Introduction
- The ileum is middle part of the intestine, important for its comprehensive study in connection with the performance of enormous functions, the separation of enzymes and the absorption of substances, minerals and salts. The ileum is located in the right lateral cavity of the abdomen, bordered by the bauginiev valve from the appendix (iliotsecal valve). The upper tuft of the intestine is vertical, the lower tuft is horizontal [2].The ileum produces an average of 2.4 liters of intestinal juice in 24 hours. Its composition is alkaline, the main part consists of enzymes, they are consist of 22 different species of the enzymes. The main part of these enzymes activates pancreatic trypsinogen [5,8]. The ileum is often affected by inflammatory diseases, and these diseases are clinically and morphologically similar to each other. Underlying the development of these diseases is a violation of the digestive, excretory, absorption and motility functions of the intestine. Therefore, the study of anatomy, topography and histotopography of the ileum is an important issue [4,7,8].
2. Purpose of the Research
- To improve the data on the anatomical, histotopographic and morphometric parameters of the ileum of infants who died from traumatic brain injury.
3. Materials and Methods
- The materials of the autopsy performed at the Department of Pediatrics of the Republican Center for Pathological Anatomy of the Ministry of Health of the Republic of Uzbekistan were taken as material. The lateral intestine was completely isolated during autopsy of infants who died from traumatic brain injury during delivery, brought from the maternity ward. It was opened, the mucous membrane surface was washed, its length was measured, and the peyer patches on the mucosal surface were counted. Pieces of 20 cm from the head, middle and last distal part of the ileum were cut and glued to a thin paper surface, the paper and intestine were rolled together, the waist was tied and placed in 10% neutralized formalin. After curing for 72 h, it was washed in running water and dehydrated in increasing concentrations of alcohols and chloroform. Then wax was added and paraffin was poured and the bricks were prepared. Histological incisions 5 μm thick were taken from the lesions and stained with hematoxylin-eosin. Under the microscope of the firm Leyka were studied on 10, 20, 40 lenses and the necessary areas were photographed. In histological preparations, intestinal wall layers were measured using an ocular micrometer in 20 visual fields. The arithmetic mean (M), error (m), and reliability level (P) of each were calculated. Quantitative indicators were statistically processed.
4. Results and Discussion
- The small and large intestines are commonly referred to as intestinum tenue mesenteriale, the average length in humans is 5 m, unlike the duodenum, which is covered by the peritoneum. There is no clear boundary between the small intestine (jejunum) and the ileum [1,2]. In newborns, the length of the ileum was found to be 78 cm to 156 cm. In boys, the mean was 118.6 ± 12.5 cm. The girls were found to be slightly shorter, averaging 104.3 ± 8.5 cm. However, it was observed that the small intestine had a larger diameter, the ileum was smaller, and the wall was thicker. Examination of the small intestinal mucosa revealed the presence of hemispherical, circular, or spiral folds. Circular folds are called Kerkring valves in the literature [5] and are composed of mucous and submucosal layers. Due to the presence of a large number of suckers in the mucous membrane of the ileum, it is anatomically similar to velvet material, microscopically the suckers are 1 mm thick. In the proximal part of the ileum, the suckers become leafy, and in the distal part they become finger-shaped. Between the teats, the tubular intestinal glands and Liberkyun glands located in the submucosal layer open the excretory openings. Cylindrical covering and goblet cells are detected on the surface of the mucous membrane, and the presence of stem, squamous, goblet, Panet and enteroendocrine cells is detected in the glands [6]. Stem cells are sucking cells, columnar, the nucleus is oval in shape, located in the basal part, with a marginal stalk on the surface. These cells synthesize disaccharidase, peptidase, hydrolyze disaccharides and dipeptides to monosaccharides and amino acids. Fats, on the other hand, are processed using pancreatic lipases and bile and are absorbed in the upper part of the duodenium and small intestine. The goblet cells are located between the squamous enterocytes, the number of which increases towards the ileum. They synthesize the sour glycoproteins of mucins to form a mucous substance. Panet cells are located in the basal part of the intestinal glands, produce lysozyme, and dissolve the outer layer of bacteria. M-cells are specific, located on the surface of lymphoid follicles, and produce numerous microinvaginations in the basement membrane, which are co-located with a large number of lymphocytes and antigen-detecting macrophages. These cells phagocytose, determine, and transmit antigens to macrophages and lymphocytes. Therefore, these cells play an important role in the intestinal immune system. Under the M-cell, the basal membrane is ruptured and provides transport of substances [3,4,5]. In the ileum there are endocrinocytes: EC-cells that synthesize serotonin, motilin, R substance, A-cell with enteroglucagon, S-cell with secterin, I-cells with cholecystokinin and pancreatosimine [3]. Intestinal folds expand the intestinal surface 3 times, suckers 10 times, microvilli 20 times, they expand a total of 600 times, and the intestinal surface is 200 m2.Microscopic examination of the ileal mucosa revealed that the surface was covered with a single-layered, in some places multilayered cylindrical epithelium, on the surface of which there are numerous small microscopic cells, basically a single line of glycocalyx stained with eosin. But this line is broken on the surface of the goblet cells, the intestinal cavity is openly connected with the goblet cell cytoplasm. The cytoplasm of the cylindrical covering epithelium is stained in granular form due to the presence of both vacuoles and eosinophilic granules. The nuclei of these cells are located mainly in the basal part of the cells, but the nuclei of some are located in the middle part of the cells. The karyoplasm of the nuclei is mainly hyperchromic, but there are also relatively lightly stained nuclei with hematoxylin. Lymphocytes, small, round in shape, dark-stained with hematoxylin nucleus, lympho-epithelial symbiosis are observed between the layers of the covering epithelium. The intermediate material of the basal membrane and connective tissue-specific plate under the covering epithelial line is found, basophilic, stained with eosin. The presence of differentiated histiocytic and lymphoid cells in the specific plate is found. The nuclei of lymphoid cells are mostly round in shape and dark stained with hematoxylin, some of which are in a state of migration through the basement membrane. The capillary wall of this layer is thin, it consists of endothelial cells and the basement membrane. The presence of eosinophilic fat cells in the cytoplasm around certain vessels is detected.
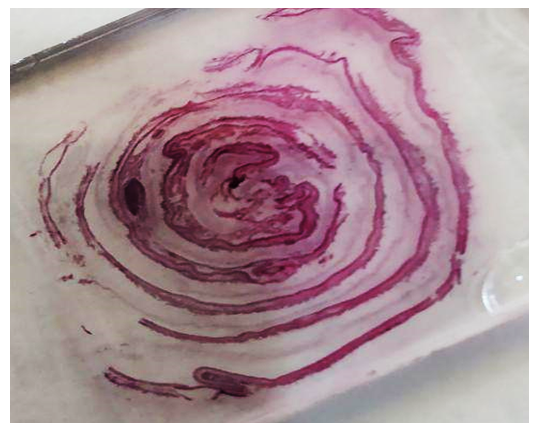 | Figure 1. Lateral intestinal wall wrapping. Paint: G-E. X: 10x100 |
|
5. Conclusions
- The average length of the ileum in newborn who died of traumatic brain injury was 118.6 ± 12.5 m in boys, shorter in girls - 104.3 ± 8.5 m, and the average number of peyer's patches was 9.4 ± 0.8 m.It was found that the epithelium covering the mucous membrane of the ileum is single-layered, in some places multi-layered, their nuclei are mainly in the basal part of the cell, but some are in the middle area, at least in the presence of goblet cells.The number of peyer's patches in the submandibular mucosa was relatively small, the lymphoid follicles in them completely occupy the submucosa and the special plate, the reticular and lymphocyte cells were sparse.While the thickness of the ileal wall averaged 26,385 ± 342 μm, almost half of it was in the mucous membrane, including the nipples and crypts, and the rest was in the submucosa, muscle, and serous membrane.