-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(12): 1020-1023
doi:10.5923/j.ajmms.20201012.19
Received: Nov. 22, 2020; Accepted: Nov. 30, 2020; Published: Dec. 15, 2020

Pathogenetic Мechanisms of Acne
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAzimova F. V., Sabirov U. Y., Khojaeva M. B., Abdurashidov A. A.
Republic Specialized Scientific-Practical Medical Center of Dermatology and Venerology Ministry of Health of the Republic of Uzbekistan, Tashkent
Correspondence to: Azimova F. V., Republic Specialized Scientific-Practical Medical Center of Dermatology and Venerology Ministry of Health of the Republic of Uzbekistan, Tashkent.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article is focused on the study of androgen receptor activity regulators in the pathogenesis of androgen-dependent dermatopathies, in particular, in acne disease - 25-OH-VD, cytochrome p 450 (17- alpha hydroxylase), insulin-like growth factor, and the study of hormonal map. There were 64 patients with acne at the age from 14 to 25 years under observation. The results of the study showed reliable disorders of enzyme regulators of androgenic receptors - 25-OH-VD, cytochrome p 450 (17- alpha hydroxylase), as well as growth factor (insulin-like growth factor), which are important in the pathogenesis of rapid non-genomic molecular-cellular reactions of metabolism of peripheral androgens and enzymes in the case of acne disease, and in the future may help develop new algorithms for the treatment of acne disease.
Keywords: Androgen-dependent dermatopathy, Etiology, Pathogenesis, Hormonal status
Cite this paper: Azimova F. V., Sabirov U. Y., Khojaeva M. B., Abdurashidov A. A., Pathogenetic Мechanisms of Acne, American Journal of Medicine and Medical Sciences, Vol. 10 No. 12, 2020, pp. 1020-1023. doi: 10.5923/j.ajmms.20201012.19.
1. Introduction
- Androgen-dependent dermatopathy is a symptomatic complex of the effect on the skin of androgens with their overproduction in the body or with increased sensitivity of sebaceous glands and hair follicles to the latter, characterized by androgenic alopecia, acne, and Seborrheic dermatitis. This symptom-complex can be considered not only a medical, but also a social and economic problem, as it leads to the development of psycho-emotional reactions that reduce the quality of life of women and, as a consequence, restrictions in the choice of profession and employment. But the degree of development of these manifestations is due not only to the concentration of androgens in the blood, but also to their peripheral metabolism at the receptor level of hair follicles. [3,14] Hair growth and sebaceous glands are affected by the most active androgen - dehydrotestosterone, which is formed as a result of testosterone metabolism under the influence of enzyme 5α-reductase at the level of hair follicles and sebaceous glands receptors. The sources of overproduction of androgens in the female body are the ovaries or adrenal glands and other extraovarian factors that occur in the neuroendocrine syndromes described before: adrenogenital syndrome, metabolic syndrome with impaired reproductive function, and polycystic ovarian syndrome [1,6].As a target tissue for androgens, the skin takes an active part in the metabolism of steroid sex hormones, in particular in the extraglandular formation of precursor steroids. In the hair follicle and sebaceous gland, as an autonomous source of hormones, there is 3β-hydroxysteroid dehydrogenase (HSD) type 1, 17β- HSD type 5 and 5α-reductase type 1, which provide conversion of dehydroepiandrosterone sequentially into Androstendon, testosterone and dehydrotestosterone. But also we found trace amount of cytochrome P450c17 in sebocytes, a key enzyme that provides an opportunity to form dehydroepiandrosterone cholesterol. [4,9].The signaling pathway of the androgen receptor includes the following stages; After testosterone penetrates the target cell, it binds to the androgen receptor either directly or after transformation into a more metabolically active form - Dehydrotestosterone - under the action of 5-alpha-reductase enzyme (Pic. 1). [25,12] The action of AR-Dehydrotestosterone complex is 3-10 times stronger than AR-Dehydrotestosterone complex (Nissar AS., Heath JA. 2008). Ligand binding to the receptor in cytoplasm causes dissociation of chaperone complexes (including heat shock proteins, namely Hsp70, Hsp90 and p23), which are at rest in the AR-related state and protect it from degradation. At the same time, conformational changes and phosphorylation take place in the receptor, as a result of which it is translocated to the nucleus. The receptor bond attracts many auxiliary factors, known as coregulators, which create favorable or unfavorable transcription conditions in the promoter region and interact with other common transcription factors and RNA polymerase II. Coactivators can be represented as adapters in the signal path. They are insulin-like growth factor - IGF1, interleukin IL - 6 (Hahn S, Haselhorst U. 2006). [3,9,13].
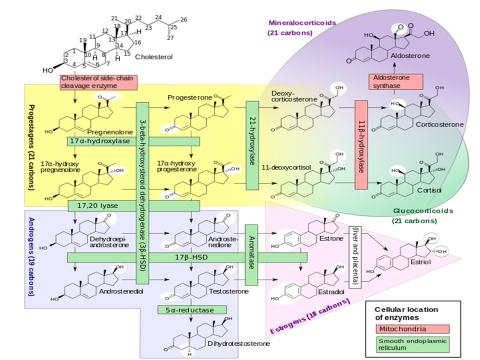 | Figure 1. Metabolism of steroid sex hormones in mitochondrion and endoplasmic reticulum |
2. Patients and Methods
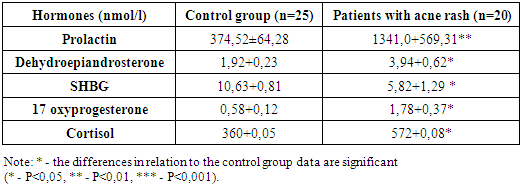
- Under our supervision there were 64 patients with acne at the age of 14-25 years. The duration of the disease was up to 1 one year in 38.2% of patients with acne, from 2 years to 3 years - in 29.1%, from 3 to 5 years - in 20%, more than 5 years - in 12.7%. Among patients with vulgar acne in 74% of cases the papulo-pustule form was registered, in 26 - the comedonic form. Papulo-pustular and pustular vulgar acne usually began in patients with acute and significant number of vulgar acne. After several days, the nodules dissolved, leaving small pigment spots or scars in their place. Induced acne (A. indurata) was typical for patients who also had dense seborrhea and androgenic alopecia. Dense, painful infiltrates, the size of a large pea or larger; the skin over which is was dyed blue. The infiltrates were successively absorbed, releasing a viscous oily-blue liquid. During healing, there were deep scars, often hypertrophic. Drainage eels? (A. confluens) were the result of the growth and fusion of inductive acne, which can merge between themselves by deep passages, forming a roller-shaped or worm-shaped infiltration, opened by several holes. Sometimes this process took a sharp current, the skin over the infiltrates was stained bright red, at the opening was released a large number of purulent content - phlegmonose acne (A. phlegmonosa). The comedonic form was expressed by open (black acne, blackheads) or closed (white acne, whiteheads) rash. Comedones were localized on the skin of the face, chest, back, and later in the ears, on the back of the neck.The open comedones had the form of black dots blocking the mouths of the hair follicles; while squeezing a thick skin fat and horny scales were distinguished. The black color of comedon is due to melanin. Closed comedones were small, slightly elevated hemispherical papules of white color and had a slight follicular opening. Closed comedones were a major potential source of inflammatory acne. Among this group of patients there were so-called sandpaper comedones. They were multiple (up to 500 pieces), small white comedones, localized mainly on the forehead; macrocomedons, which are large, more than 1 mm in diameter, closed or open (often closed) comedones. Sandpaper comedons and macrocomedons were not treated as usual; the so-called "submarine comedones" are large comedon-like structures up to 0.5 cm in diameter, located in deep parts of the dermis. They are the source of recurring inflammatory nodes. All patients with acne were determined the concentrations of hormones in the blood - Dehydroepiandrosterone, SHBG, Cortisol, Prolactin and 17 Oxyprogesterone radioimmunological method using commercial sets of "Déifia" (Finland) on the device "WallacOy" (Finland), using as a label heavy metal europium. Research in blood 25-OH-VD, cytochrome p 450 (17- alphahydroxylase), insulin-like growth factor was carried out on "HumareaderSingle" by the automated immunoenzyme method.
3. Results and Discussion
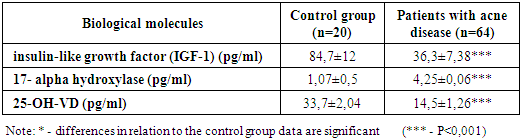
- A study of cytochrome p 450 (17- alpha hydroxylase), which is an enzyme-catalyst for the synthesis of Dehydroepiandrosterone from cholesterol, in all patients with acne disease was significantly increased - 4.25±0.060 pg/ml (P <0.001), while in control group patients was 1.07±0.5 pg/ml (P <0.001), alpha-hydroxylase is a human enzyme encoded with the CYP17A1 gene ("cytochrome P450, family 17, subfamily A, polypeptide 1") on the 10th chromosome. By catalyzing the addition of hydroxyl group to pregnenolone and progesterone in the position of the 17th carbon atom, 17-alpha-hydroxyxylase promotes their transformation into 17-hydroxypregnenolone and 17-hydroxyprogesterone, respectively. The same enzyme acts as a lyase by cutting the bond between 17 and 20 carbon (see the scheme of numbering) in the molecules of 17-hydroxypregnenolone and 17-hydroxyprogesterone and thus forming Dehydroepiandrosterone and Androstendon. In this group of patients, the 25-ON-VD index, which determines the direct correlation with the concentration of the globulin binding sex steroids and the reverse – with the index of free androgens, was significantly lower - 14.5±1.26 pg/ml (P <0.001) compared to the same index of the control group 33.7±2.04 pg/ml. The study of insulin-like growth factor as a coactivator and adapter on the way of mitosis signal transmission and differentiation to the cell in a patient with acne disease showed a reliable decrease - 36.3±7.38 pg/ml (P <0.001), while in the control group patients the similar index was 84.7±12 pg/ml (Table 1).
|
|
4. Conclusions
- Therefore, androgenic receptor regulators - 25-OH-VD, cytochrome p 450 (17- alpha hydroxylase), insulin-like growth factor are important in the pathogenesis of rapid non-genomic molecular-cellular metabolic reactions of peripheral androgens and, in the future, may help to determine new algorithms of acne therapy. The revealed disturbed hormonal card parameters in 32% of acne patients determine the necessity to prescribe new drugs with anti-androgenic effect, which will not only contribute to the reduction of Androstendon and Dehydroepiandrosterone sulfate in the ovaries and adrenal glands, but also block the hypersensitivity of sebaceous glands to androgens.